

Changes in the use of do-not-resuscitate orders after implementation of the Patient Self-Determination Act
- PMID: 12795732
- PMCID: PMC1494855
- DOI: 10.1046/j.1525-1497.2003.20522.x
Changes in the use of do-not-resuscitate orders after implementation of the Patient Self-Determination Act
Abstract
Objective: To determine changes in the use of do-not-resuscitate (DNR) orders and mortality rates following a DNR order after the Patient Self-determination Act (PSDA) was implemented in December 1991.
Design: Time-series.
Setting: Twenty-nine hospitals in Northeast Ohio.
Patients/participants: Medicare patients (N = 91,539) hospitalized with myocardial infarction, heart failure, gastrointestinal hemorrhage, chronic obstructive pulmonary disease, pneumonia, or stroke.
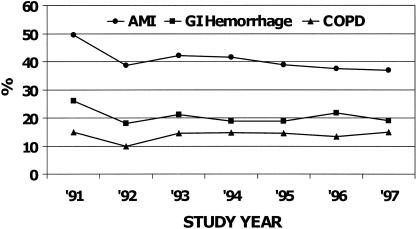
Measurements and main results: The use of "early" (first 2 hospital days) and "late" DNR orders was determined from chart abstractions. Deaths within 30 days after a DNR order were identified from Medicare Provider Analysis and Review files. Risk-adjusted rates of early DNR orders increased by 34% to 66% between 1991 and 1992 for 4 of the 6 conditions and then remained flat or declined slightly between 1992 and 1997. Use of late DNR orders declined by 29% to 53% for 4 of the 6 conditions between 1991 and 1997. Risk-adjusted mortality during the 30 days after a DNR order was written did not change between 1991 and 1997 for 5 conditions, but risk-adjusted mortality increased by 21% and 25% for stroke patients with early DNR and late DNR orders, respectively.
Conclusions: Overall use of DNR orders changed relatively little after passage of the PSDA, because the increase in the use of early DNR orders between 1991 and 1992 was counteracted by decreasing use of late DNR orders. Risk-adjusted mortality rates after a DNR order generally remained stable, suggesting that there were no dramatic changes in quality of care or aggressiveness of care for patients with DNR orders. However, the increasing mortality for stroke patients warrants further examination.
Figures
Comment in
-
Virtual physicians, health systems, and the healing relationship.J Gen Intern Med. 2003 May;18(5):404-6. doi: 10.1046/j.1525-1497.2003.30348.x. J Gen Intern Med. 2003. PMID: 12795741 Free PMC article. No abstract available.
Similar articles
-
Trends in postdischarge mortality and readmissions: has length of stay declined too far?Arch Intern Med. 2004 Mar 8;164(5):538-44. doi: 10.1001/archinte.164.5.538. Arch Intern Med. 2004. PMID: 15006831
-
Outcomes of patients with do-not-resuscitate orders. Toward an understanding of what do-not-resuscitate orders mean and how they affect patients.Arch Intern Med. 1995 Oct 23;155(19):2063-8. Arch Intern Med. 1995. PMID: 7575065
-
Adjustment for do-not-resuscitate orders reverses the apparent in-hospital mortality advantage for minorities.Am J Med. 2005 Apr;118(4):400-8. doi: 10.1016/j.amjmed.2005.01.008. Am J Med. 2005. PMID: 15808138
-
Do-not-resuscitate orders in suicidal patients: clinical, ethical, and legal dilemmas.Psychosomatics. 2010 Jul-Aug;51(4):277-82. doi: 10.1176/appi.psy.51.4.277. Psychosomatics. 2010. PMID: 20587754 Review.
-
[Ethical conflicts during anesthesia. "Do not resuscitate" orders in the operating room].Anaesthesist. 1997 Apr;46(4):267-74. doi: 10.1007/s001010050400. Anaesthesist. 1997. PMID: 9229979 Review. German.
Cited by
-
The epidemiology of do-not-resuscitate orders in patients with trauma: a community level one trauma center observational experience.Scand J Trauma Resusc Emerg Med. 2015 Feb 3;23:9. doi: 10.1186/s13049-015-0094-2. Scand J Trauma Resusc Emerg Med. 2015. PMID: 25645242 Free PMC article.
-
Development and evaluation of an aged care specific Advance Care Plan.BMJ Support Palliat Care. 2013 Jun;3(2):188-95. doi: 10.1136/bmjspcare-2012-000392. Epub 2013 Mar 15. BMJ Support Palliat Care. 2013. PMID: 23626906 Free PMC article.
-
Virtual physicians, health systems, and the healing relationship.J Gen Intern Med. 2003 May;18(5):404-6. doi: 10.1046/j.1525-1497.2003.30348.x. J Gen Intern Med. 2003. PMID: 12795741 Free PMC article. No abstract available.
-
Terminal hospitalizations of nursing home residents: does facility increasing the rate of do not resuscitate orders reduce them?J Pain Symptom Manage. 2011 Jun;41(6):1040-7. doi: 10.1016/j.jpainsymman.2010.07.014. Epub 2011 Jan 28. J Pain Symptom Manage. 2011. PMID: 21276698 Free PMC article.
-
Electronic screening of dictated reports to identify patients with do-not-resuscitate status.J Am Med Inform Assoc. 2004 Sep-Oct;11(5):403-9. doi: 10.1197/jamia.M1518. Epub 2004 Jun 7. J Am Med Inform Assoc. 2004. PMID: 15187069 Free PMC article.
References
-
- Wenger NS, Pearson ML, Desmond KA, Kahn KL. Changes over time in the use of do not resuscitate orders and the outcomes of patients receiving them. Med Care. 1997;35:311–9. - PubMed
-
- Jayes RL, Zimmerman JE, Wagner DP, Draper EA, Knaus WA. Do-not-resuscitate orders in intensive care units. Current practices and recent changes. JAMA. 1993;270:2213–7. - PubMed
-
- Jonsson PV, Mc Namee M, Campion EW. The ‘do not resuscitate’ order. A profile of its changing use. Arch Intern Med. 1988;148:2373–5. - PubMed
-
- Stern SG, Orlowski JP. DNR or CPR–the choice is ours. Crit Care Med. 1992;20:1263–72. - PubMed
-
- Omnibus Budget Reconciliation Act of 1990. Public law no. 101–508. 2002. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources