

Surgical adverse events, risk management, and malpractice outcome: morbidity and mortality review is not enough
- PMID: 12796581
- PMCID: PMC1514679
- DOI: 10.1097/01.SLA.0000072267.19263.26
Surgical adverse events, risk management, and malpractice outcome: morbidity and mortality review is not enough
Abstract
Objective: To review all admissions (age > 13) to three surgical patient care centers at a single academic medical center between January 1, 1995, and December 6, 1999, for significant surgical adverse events.
Summary background data: Little data exist on the interrelationships between surgical adverse events, risk management, malpractice claims, and resulting indemnity payments to plaintiffs. The authors hypothesized that examination of this process would identify performance improvement opportunities overlooked by standard medical peer review; the risk of litigation would be constant across the three homogeneous patient care centers; and the risk management process would exceed the performance improvement process.
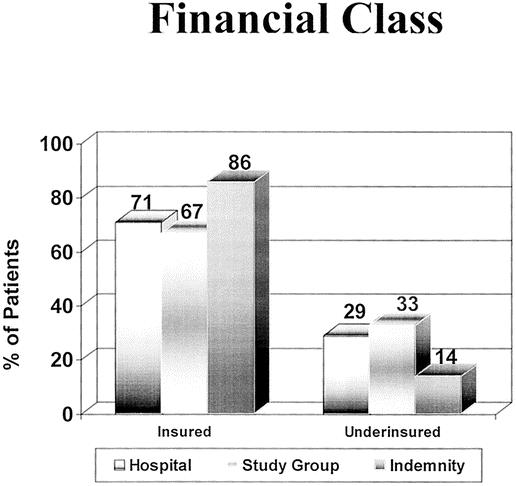
Methods: Data collected included patient demographics (age, gender, and employment status), hospital financials (hospital charges, costs, and financial class), and outcome. Outcome categories were medical (disability: <1 month, 1-6 months, permanent/death), legal (no legal action, settlement, summary judgment), financial (indemnity payments, legal fees, write-offs), and cause and effect analysis. Cause and effect analysis attempts to identify system failures contributing to adverse outcomes. This was determined by two independent analysts using the 17 Harvard criteria and subdividing these into subsystem causative factors.
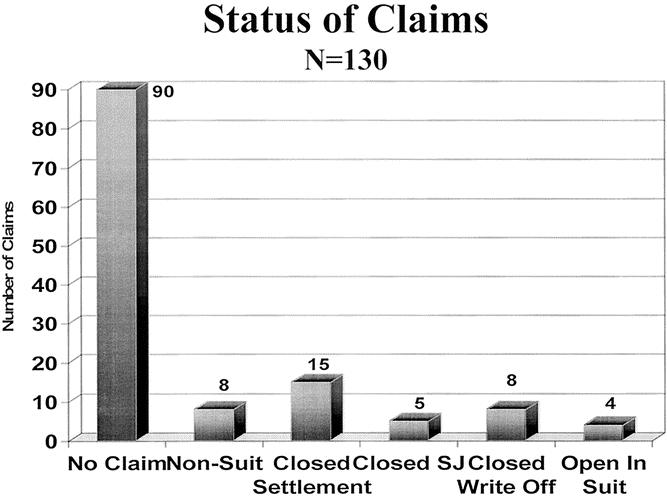
Results: The study group consisted of 130 patients with surgical adverse events resulting in total liabilities of $8.2 million US dollars. The incidence of adverse events per 1,000 admissions across the three patient care centers was similar, but indemnity payments per 1,000 admissions varied (cardiothoracic = $30 US dollars, women's health = $90 US dollars, trauma = $520 US dollars). Patient demographics were not predictive of high-risk subgroups for adverse events or litigation. In terms of medical outcome, 51 patients had permanent disability or death, accounting for 98% of the indemnity payments. In terms of legal outcome, 103 patients received no indemnity payments, 15 patients received indemnity payments, four suits remain open, and in eight cases charges were written off ($0.121 million US dollars). To date, no cases have been adjudicated in court. Cause and effect analysis identified 390 system failures contributing to the adverse events (mean 3.0 failures per adverse event); there were 4.7 failures per adverse event in the 15 indemnity cases. Five categories of causes accounted for 75% of the failures (patient management, n = 104; communication, n = 89; administration, n = 33; documentation, n = 32; behavior, n = 23). The current medical review process would have identified 104 of 390 systems failures (37%).
Conclusions: This study demonstrates no rational link between the tort system and the reduction of adverse events. Sixty-three percent of contributing causes to adverse events were undetected by current medical review processes. Adverse events occur at the interface between different systems or disciplines and result from multiple failures. Indemnity costs per hospital day vary dramatically by patient care center (range $3.60-97.60 US dollars a day). The regionalization of healthcare is in jeopardy from the burden of high indemnity payments.
Figures
Similar articles
-
An epidemiologic study of closed emergency department malpractice claims in a national database of physician malpractice insurers.Acad Emerg Med. 2010 May;17(5):553-60. doi: 10.1111/j.1553-2712.2010.00729.x. Acad Emerg Med. 2010. PMID: 20536812
-
Cause and effect analysis of closed claims in obstetrics and gynecology.Obstet Gynecol. 2005 May;105(5 Pt 1):1031-8. doi: 10.1097/01.AOG.0000158864.09443.77. Obstet Gynecol. 2005. PMID: 15863541
-
Claims, errors, and compensation payments in medical malpractice litigation.N Engl J Med. 2006 May 11;354(19):2024-33. doi: 10.1056/NEJMsa054479. N Engl J Med. 2006. PMID: 16687715
-
Perioperative Complications in Obstructive Sleep Apnea Patients Undergoing Surgery: A Review of the Legal Literature.Anesth Analg. 2016 Jan;122(1):145-51. doi: 10.1213/ANE.0000000000000841. Anesth Analg. 2016. PMID: 26111263 Review.
-
[Patient safety and risk management].Med Klin (Munich). 2005 Aug 15;100(8):478-85. doi: 10.1007/s00063-005-1061. Med Klin (Munich). 2005. PMID: 16096729 Review. German.
Cited by
-
Medical Malpractice in Nerve Injury of the Upper Extremity.Hand (N Y). 2021 Jul;16(4):425-431. doi: 10.1177/1558944720906500. Epub 2020 Feb 28. Hand (N Y). 2021. PMID: 32108518 Free PMC article.
-
Human Factors Integration in Robotic Surgery.Hum Factors. 2024 Mar;66(3):683-700. doi: 10.1177/00187208211068946. Epub 2022 Mar 5. Hum Factors. 2024. PMID: 35253508 Free PMC article. Review.
-
Professional liability in orthopaedics and traumatology in Italy.Clin Orthop Relat Res. 2013 Oct;471(10):3349-57. doi: 10.1007/s11999-013-3165-6. Epub 2013 Jul 16. Clin Orthop Relat Res. 2013. PMID: 23857317 Free PMC article.
-
Complement C1 esterase inhibitor levels linked to infections and contaminated heparin-associated adverse events.PLoS One. 2012;7(4):e34978. doi: 10.1371/journal.pone.0034978. Epub 2012 Apr 13. PLoS One. 2012. PMID: 22514695 Free PMC article.
-
Can Surgeons Adequately Capture Adverse Events Using the Spinal Adverse Events Severity System (SAVES) and OrthoSAVES?Clin Orthop Relat Res. 2017 Jan;475(1):253-260. doi: 10.1007/s11999-016-5021-y. Epub 2016 Aug 10. Clin Orthop Relat Res. 2017. PMID: 27511203 Free PMC article.
References
-
- Cox T. Doctors facing dilemma. Charleston Daily Mail. April 10, 2002.
-
- Pennsylvania Medical Society press release; www.pamsmed.org.
-
- Rivera P. Malpractice rates take a feverish leap: Texas doctors hit hard by increases, which insurers say are needed. Dallas Morning News. Jan. 20, 2002.
-
- Booth W. Las Vegas trauma center closes as doctors quit; surgeon cite rising costs of malpractice insurance, lawsuits. A growing problem. Washington Post. July 4, 2002.
-
- Warner J, Advanti P, Large A. Managing health care malpractice costs. The Advisory Board, June 2002.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
