

Influence of transfusions on perioperative and long-term outcome in patients following hepatic resection for colorectal metastases
- PMID: 12796583
- PMCID: PMC1514683
- DOI: 10.1097/01.SLA.0000072371.95588.DA
Influence of transfusions on perioperative and long-term outcome in patients following hepatic resection for colorectal metastases
Abstract
Objective: To determine if transfusion affected perioperative and long-term outcome in patients undergoing liver resection for metastatic colorectal cancer.
Summary background data: Blood transfusion produces host immunosuppression and has been postulated to result in adverse outcome for patients undergoing surgical resection of malignancies.
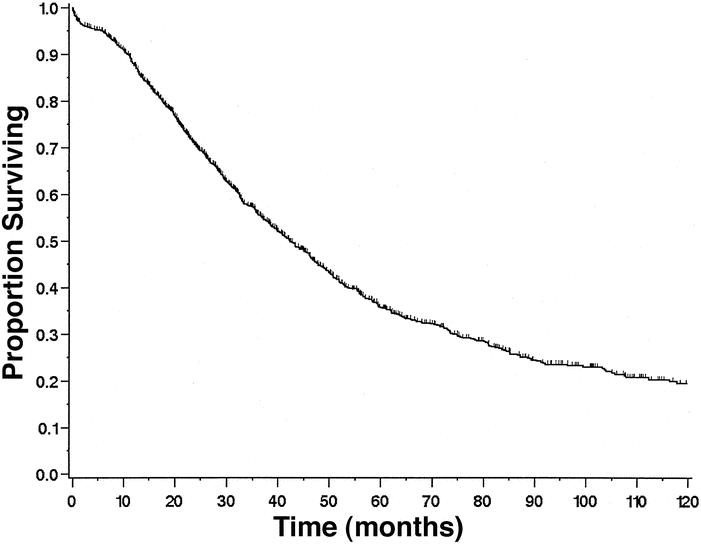
Methods: Blood transfusion records and clinical outcomes for 1,351 patients undergoing liver resection at a tertiary cancer referral center were analyzed.
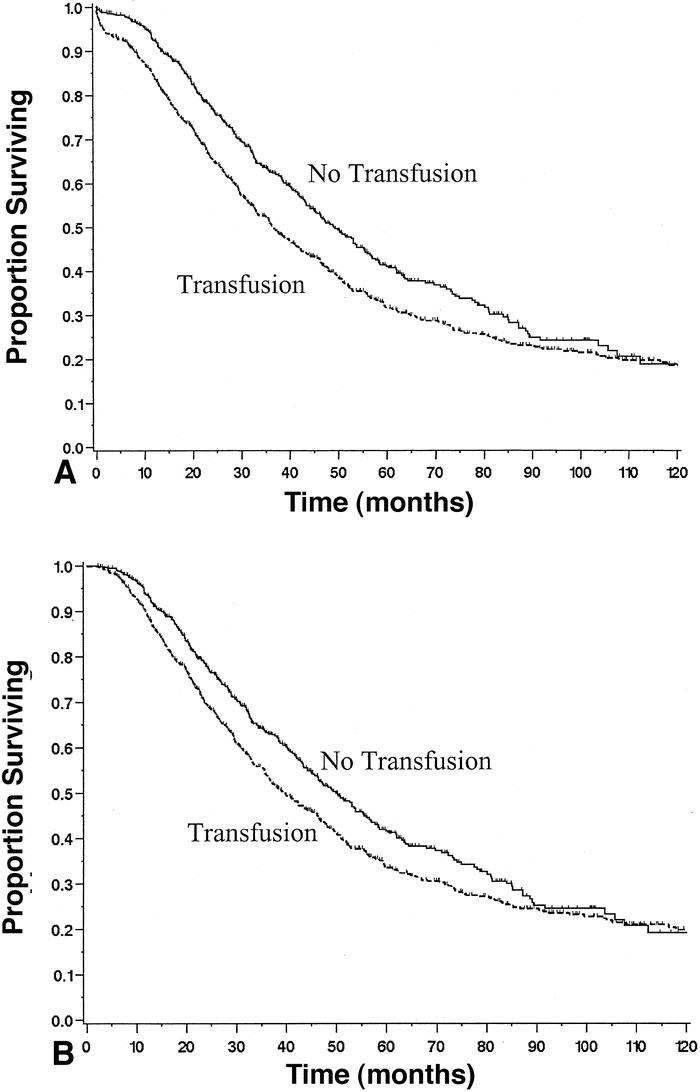
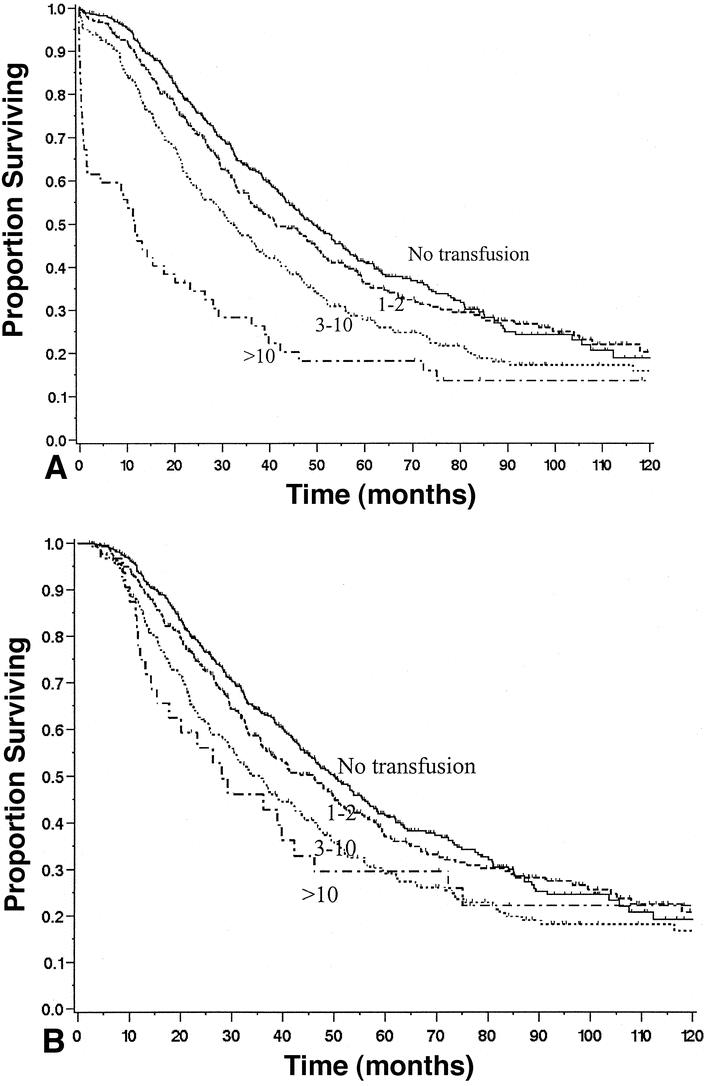
Results: Blood transfusion was associated with adverse outcome after liver resection. The greatest effect was in the perioperative course, where transfusion was an independent predictor of operative mortality, complications, major complications, and length of hospital stay. This effect was dose-related. Patients receiving one or two units or more than two units had an operative mortality of 2.5% and 11.1%, respectively, compared to 1.2% for patients not requiring transfusions. Transfusion was also associated with adverse long-term survival by univariate analysis, but this factor was not significant on multivariate analysis. Even patients receiving only one or two units had a more adverse outcome.
Conclusions: Perioperative blood transfusion is a risk factor for poor outcome after liver resection. Blood conservation methods should be used to avoid transfusion, especially in patents currently requiring limited amounts of transfused blood products.
Figures
Comment in
-
Influence of transfusions on perioperative and long-term outcome in patients following hepatic resection for colorectal metastases.Ann Surg. 2005 Feb;241(2):381. doi: 10.1097/01.sla.0000152989.76942.6b. Ann Surg. 2005. PMID: 15650652 Free PMC article. No abstract available.
References
-
- Gascon P, Zoumbos NC, Young NS. Immunological abnormalities in patients receiving multiple blood transfusions. Ann Intern Med. 1984; 100: 173–177. - PubMed
-
- Kaplan J, Sarnaik S, Gitlin J, et al. Diminished helper/suppressor lymphocyte ratios and natural killer activity in recipients of repeated blood transfusions. Blood. 1984; 64: 308–310. - PubMed
-
- Peters WR, Fry RD, Fleshman JW, et al. Multiple blood transfusions reduce the recurrence rate of Crohn’s disease. Dis Colon Rectum. 1989; 32: 749–753. - PubMed
-
- Ghio M, Contini P, Mazzei C, et al. Soluble HLA class I, HLA class II, and Fas ligand in blood components: A possible key to explain the immunomodulatory effects of allogeneic blood transfusions. Blood. 1999; 93: 1770–1777. - PubMed
-
- Burrows L, Tartter P. Effect of blood transfusions on colonic malignancy recurrence rate. Lancet. 1982; 2: 662. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
