

Complex blunt aortic injury or repair: beneficial effects of cardiopulmonary bypass use
- PMID: 12796585
- PMCID: PMC1514682
- DOI: 10.1097/01.SLA.0000071566.43029.E0
Complex blunt aortic injury or repair: beneficial effects of cardiopulmonary bypass use
Abstract
Objective: To compare the outcomes and associated morbidity in patients with blunt aortic injury (BAI) repaired using cardiopulmonary bypass versus no bypass. Special consideration is given to the influence of bypass in the outcome of complex injuries or repair circumstances.
Summary background data: There are conflicting data concerning the utility of bypass techniques in the operative management of BAI, and controversy over the subject persists. During the last decade, surgeons at the authors' institution have undergone a change in philosophy concerning management of these injuries and began almost exclusively using cardiopulmonary bypass for the repair in 1996. This project explores the effects of this change in the management of BAI.
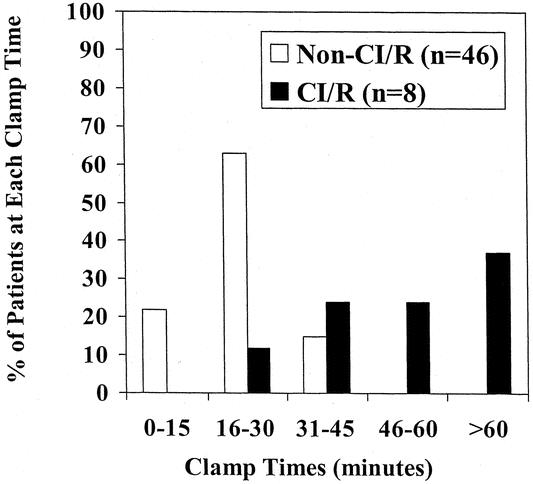
Methods: The records of all patients with BAI admitted to a level 1 trauma center over a period of 12 years were reviewed for demographics, injury characteristics, operative technique, and outcome. The bypass group was compared to the no bypass group with respect to morbidity and mortality. Those with a complex injury or repair (CI/R) were examined as a subgroup. CI/R was defined as the presence of an injury with extension proximal to the subclavian artery, involvement of branch vessels, or requirement of maneuvers interfering with anastomosis construction, such as cardiac massage.
Results: From January 1, 1990, to December 31, 2001, 91 patients were admitted to Wake Forest University Baptist Medical Center with BAI. Sixty-five of these underwent operative repair. Sixty (32 no bypass, 28 bypass) survived to the immediate postoperative period. Injury Severity Score was similar (33 no bypass, 31 bypass, P =.48), as was admission base deficit (-9.2 m Eq/L no bypass vs. -7.0 mEq/L B, P =.13). Paraplegia occurred in four (12%) of the no bypass group as opposed to 0 of the bypass group (P =.05). No patient in the bypass group experienced complications related to heparinization, and two (7%) experienced bypass-related complications (cerebral edema, femoral vein laceration). Mean clamp time for the entire group was 27 minutes. Examination of the 10 patients with CI/R who survived the operating room showed markedly longer clamp times (59 minutes vs. 22 minutes, P <.0001) and a higher rate of paraplegia/paresis (30% vs. 2%, P =.01) as compared to those without CI/R. Logistic regression demonstrated a significant relationship between increasing clamp time and the CI/R classification (P =.007). All three (100%) of the CI/R patients repaired via clamp-and-sew technique developed paraplegia, while none of the seven CI/R patients repaired on bypass developed neurologic changes (P =.008).
Conclusions: With the use of cardiopulmonary bypass in the repair of BAI, the incidence of paraplegia/paresis has fallen. While patients with typical injuries and uncomplicated repair can expect good results with either technique, cardiopulmonary bypass provides significant advantages in the repair of those with CI/R. With the use of bypass, no CI/R patient developed paraplegia, while all CI/R patients experienced paraplegia before bypass use. Although others have reported the importance of clamp time, in this series clamp time appeared largely to be a surrogate variable for complexity of injury.
Figures
Similar articles
-
Blunt aortic injury with concomitant intra-abdominal solid organ injury: treatment priorities revisited.J Trauma. 2002 Sep;53(3):442-5; discussion 445. doi: 10.1097/00005373-200209000-00008. J Trauma. 2002. PMID: 12352478
-
Favorable Outcomes of Open Surgical Repair for Blunt Aortic Injury in the Era of Endovascular Repair.Thorac Cardiovasc Surg. 2017 Mar;65(2):105-111. doi: 10.1055/s-0035-1571193. Epub 2016 Jan 28. Thorac Cardiovasc Surg. 2017. PMID: 26820450
-
Prospective study of blunt aortic injury: Multicenter Trial of the American Association for the Surgery of Trauma.J Trauma. 1997 Mar;42(3):374-80; discussion 380-3. doi: 10.1097/00005373-199703000-00003. J Trauma. 1997. PMID: 9095103 Clinical Trial.
-
Traumatic rupture of the thoracic aorta: cohort study and systematic review.J Vasc Surg. 2001 Dec;34(6):1029-34. doi: 10.1067/mva.2001.120036. J Vasc Surg. 2001. PMID: 11743556
-
Reduced mortality, paraplegia, and stroke with stent graft repair of blunt aortic transections: a modern meta-analysis.J Vasc Surg. 2008 Mar;47(3):671-5. doi: 10.1016/j.jvs.2007.08.031. Epub 2007 Nov 5. J Vasc Surg. 2008. PMID: 17980541 Review.
Cited by
-
Surgical management of chest injuries in patients with multiple and/or severe trauma- a systematic review and clinical practice guideline update.Eur J Trauma Emerg Surg. 2024 Oct;50(5):2061-2071. doi: 10.1007/s00068-024-02556-1. Epub 2024 Jun 18. Eur J Trauma Emerg Surg. 2024. PMID: 38888790 Free PMC article.
-
[Emergency surgery for chest injuries in the multiply injured: a systematic review].Unfallchirurg. 2006 Jun;109(6):447-52. doi: 10.1007/s00113-005-1048-3. Unfallchirurg. 2006. PMID: 16773318 German.
-
Endovascular approach to acute aortic trauma.World J Radiol. 2009 Dec 31;1(1):50-62. doi: 10.4329/wjr.v1.i1.50. World J Radiol. 2009. PMID: 21160721 Free PMC article.
-
Thoracic Trauma: Current Approach in Emergency Medicine.Clin Pract. 2024 Sep 10;14(5):1869-1885. doi: 10.3390/clinpract14050148. Clin Pract. 2024. PMID: 39311298 Free PMC article. Review.
-
Current management of traumatic rupture of the descending thoracic aorta.Curr Cardiol Rev. 2009 Aug;5(3):187-95. doi: 10.2174/157340309788970324. Curr Cardiol Rev. 2009. PMID: 20676277 Free PMC article.
References
-
- Smith RS, Chang FC. Traumatic rupture of the aorta: still a lethal injury. Am J Surg. 1986; 152: 660–663. - PubMed
-
- Passaro E, Pace WB. Traumatic rupture or the aorta. Surgery. 1959; 46: 787. - PubMed
-
- Lee RB, Stahkman GC, Sharp KW. Treatment priorities in patients with traumatic rupture of the thoracic aorta. Am Surg. 1992; 58: 37–43. - PubMed
-
- Cowley RA, Turney SZ, Hankins JR. Rupture of the thoracic aorta caused by blunt trauma. J Thorac Cardiovasc Surg. 1990; 100: 652–660. - PubMed
-
- Hunt JP, Baker CC, Lentz CW, et al. Thoracic aorta injuries: management and outcome of 144 patients. J Trauma. 1996; 40: 547–556. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
