

A case-cohort study for the disease natural history of adenoma-carcinoma and de novo carcinoma and surveillance of colon and rectum after polypectomy: implication for efficacy of colonoscopy
- PMID: 12799628
- PMCID: PMC2741116
- DOI: 10.1038/sj.bjc.6601007
A case-cohort study for the disease natural history of adenoma-carcinoma and de novo carcinoma and surveillance of colon and rectum after polypectomy: implication for efficacy of colonoscopy
Abstract
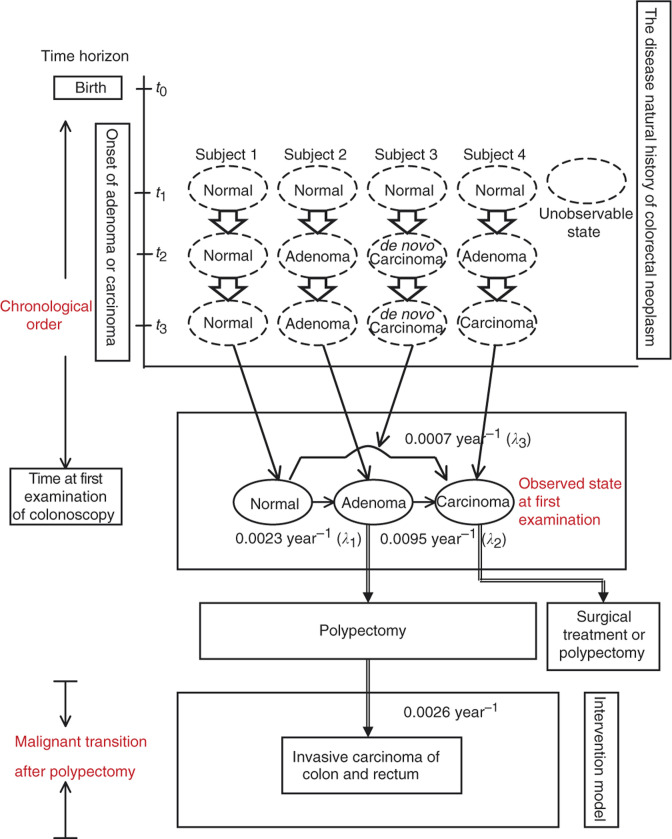
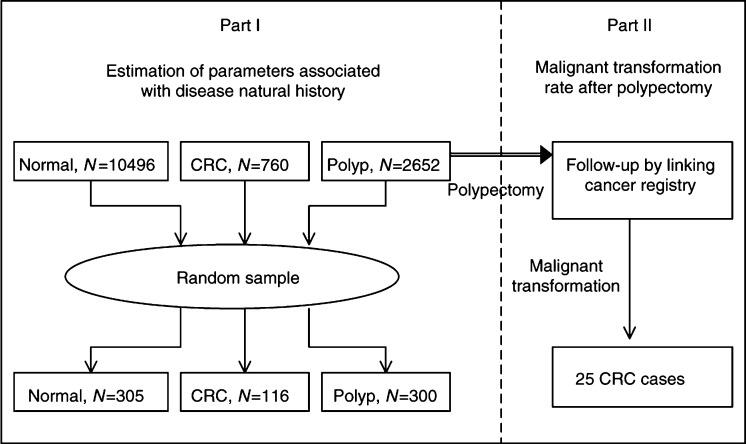
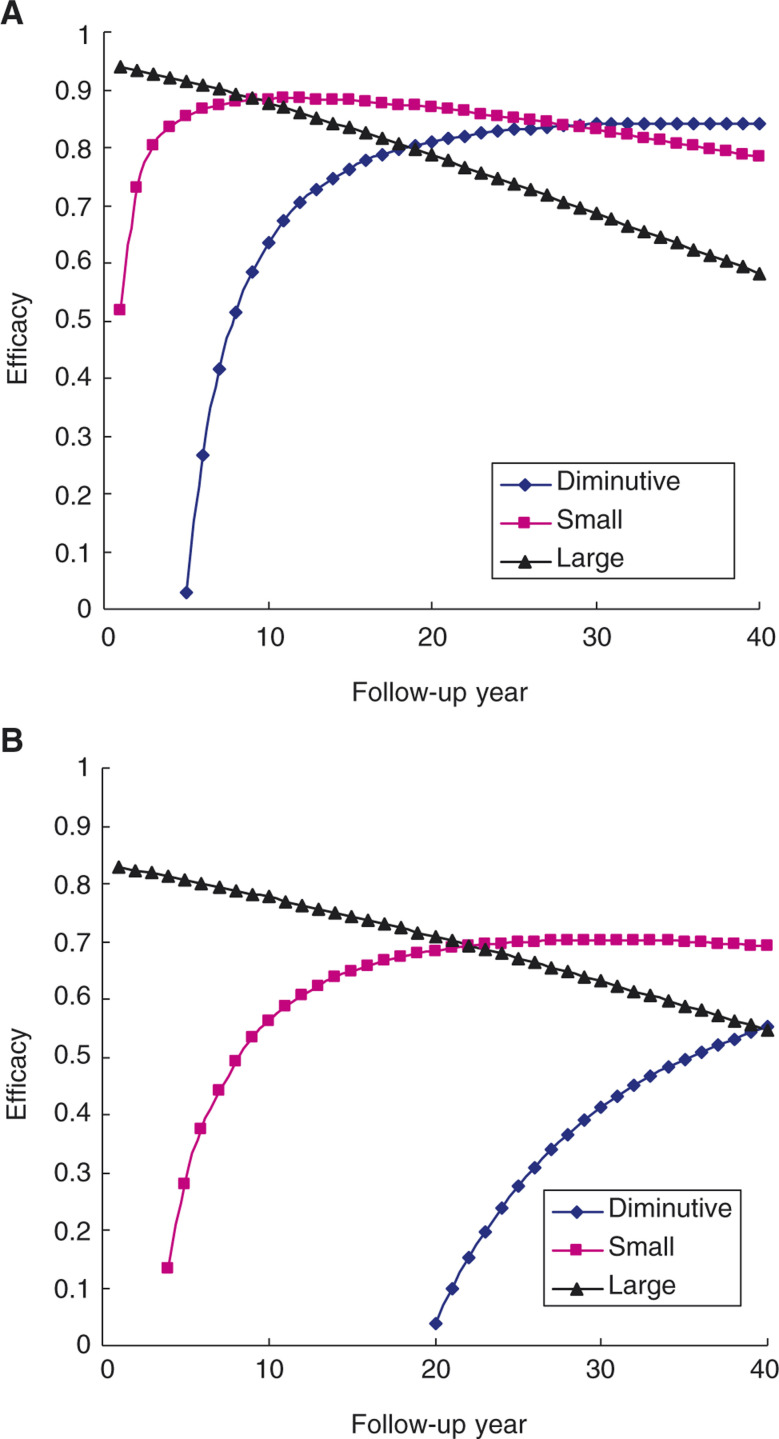
The disease natural history of colorectal neoplasm regarding two opposing theories, adenoma-carcinoma sequence and de novo carcinoma theory, is controversial and rarely quantified. The aims of this study are therefore to estimate the dwelling times of adenoma-carcinoma sequence by adenoma size and histological type, taking de novo carcinoma into account. The efficacy of polypectomy was therefore estimated making allowance for two pathways. A case-cohort design, underpinning a cohort with 13 908 subjects (including 10 496 normal subjects, 2652 polyps, 760 colorectal cancers) who underwent the first examination of colonoscopy between 1979 and 1998, was devised to estimate parameters associated with two opposing theories by randomly selecting 305 normal subjects, 300 patients with polyps, and 116 colorectal cancers from the cohort. All the 2652 polyps were linked to national cancer registry to ascertain 25 invasive carcinomas after polypectomy. For the five-state model associated with adenoma size, dwelling times of small (0.6-1 cm) and large adenoma (>1 cm) are 7.75 and 5.27 years for the model without considering de novo, and 17.48 and 15.90 years for the model taking de novo carcinoma into account. Similar findings are observed for the model associated with histological type. The estimated proportions of de novo carcinoma are 31.87% from the model by adenoma size and 27.81% from the model by histological type. Compared to size less than 5 mm, patients with adenoma size between 6 and 10 mm and patients with adenoma size larger than 1 cm have 2.17-fold (0.67-10.74) and 4.25-fold (1.23-14.70), respectively, for the risk of malignant transformation. There are similar findings for the model by histological type. The estimates of overall efficacy of colonoscopy in reducing CRC is 73% for the model allowing for de novo carcinoma and 88% for the model without considering de novo carcinoma theory. The efficacy of diminutive adenoma and small adenoma increases with follow-up years, whereas the efficacy of large adenoma decreases with follow-up years. In conclusion, about 30% of cancers arising from de novo sequence are demonstrated. This finding, together with the adenoma-carcinoma sequence associated with adenoma size and histological type, is important for the estimation of dwelling times, the efficacy of colonoscopy, and the surveillance of polyp after polypectomy.
Figures
References
-
- Bedenne L, Faivre J, Boutron MC, Piard F, Cauvin JM, Hillon P (1992) Adenoma–carcinoma sequence of ‘de novo’ carcinogenesis. A study of adenomatous remnants in a population-based series of large bowel cancer. Cancer 69: 883–888 - PubMed
-
- Chen THH, Kuo HS, Yen MF, Lai MS, Tabar L, Duffy SW (2000) Estimation of sojourn time in chronic disease screening without data on interval cases. Biometrics 56: 167–172 - PubMed
-
- Collett D (1994) Modelling survival data in medical research. pp. 199–236. Chapman & Hill, London
-
- Duffy SW, Chen HH, Tabar L, Day NE (1995) Estimation of mean sojourn time in breast cancer screening using a Markov chain model of both entry to and exit from the preclinical detectable phase. Stat Med 14: 1531–1543 - PubMed
-
- Hirota S, Kudo S, Hosobe, Kobayashi T, Himori M, Ikeka M, Takemoto Y, Nomoto M, Aoyagi Y, Asakura H (1995) P53 immunoreactive stain and early colorectal adenocarcinoma. Eur J Cancer 31: 2220–2222 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
