

Repetitive task practice: a critical review of constraint-induced movement therapy in stroke
- PMID: 12801434
- PMCID: PMC3572508
- DOI: 10.1097/01.nrl.0000031014.85777.76
Repetitive task practice: a critical review of constraint-induced movement therapy in stroke
Abstract
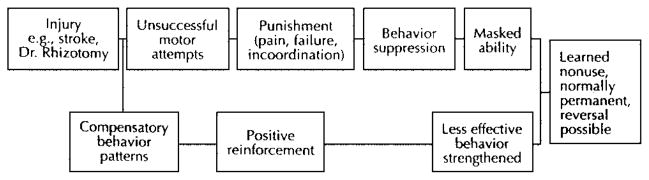
Background: Constraint-induced (CI) movement therapy (also called forced use by some investigators and clinicians) has gained increasing popularity as a treatment mode for restoring function in the upper extremities of patients with stroke. The purpose of this article is to review the concept of constraint-induced movement therapy and provide a critical analysis of the existing data.
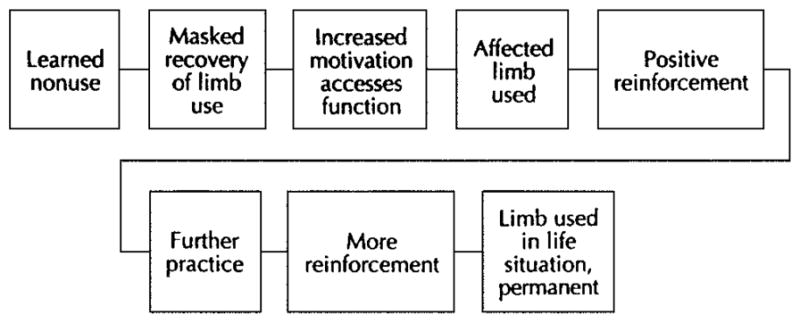
Review summary: The evidence to date offers encouragement for the application of this procedure for patients who have some movement recovery out of synergy. Success may be contingent on patient cooperation and intense repetitive use with applications of retraining through practice and shaping. The extent to which each of the latter elements influences the magnitude of recovery is still unclear. However, task novelty and challenge seem important to recovery of function. There are several methods used to map cortical changes after stroke. At this time, transcranial magnetic stimulation is the primary vehicle used to assess motor cortical reorganization after CI therapy in humans.
Conclusions: Accumulating data indicate that the size of a cortical area representative of a muscle does expand and its center of gravity does change with CI therapy.
Figures
References
-
- Gordon J. Assumptions underlying physical therapy intervention: theoretical and historical perspectives. In: Carr J, Shepherd R, editors. Movement Science: Foundations for Physical Therapy in Rehabilitation. Rockville: Aspen Publishers; 1987. pp. 1–30.
-
- Horak FB. Assumptions underlying motor control for neurologic rehabilitation: contemporary management of motor control problems. Proceedings of the II Step Conference; Alexandria, VA: APTA; 1991. pp. 11–27.
-
- Shumway-Cook A, Woollacott M. Motor Control: Theory and Practical Applications. Baltimore: Williams and Wilkins; 1995.
-
- Kwakkel G, Kollen BJ, Wagenaar RC. Therapy impact on functional recovery in stroke. Physiotherapy. 1999;85:377–391.
-
- Gelber DA, Josefczyk PB, Herrman D, et al. Comparison of two therapy approaches in the rehabilitation of the pure motor hemiparetic stroke patient. J Neurol Rehabil. 1995;9:191–196.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
