

Test characteristics of orthoptic screening examination in 3 year old kindergarten children
- PMID: 12812897
- PMCID: PMC1771738
- DOI: 10.1136/bjo.87.7.909
Test characteristics of orthoptic screening examination in 3 year old kindergarten children
Erratum in
- Br J Ophthalmol. 2003 Sep;87(9):1196
Abstract
Aim: To analyse the test characteristics of orthoptic screening for amblyopia or amblyogenic risk factors (target conditions) in kindergarten.
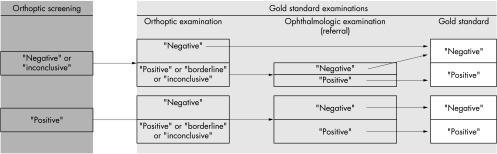
Methods: 1180 three year old children were screened by orthoptists in 121 German kindergartens. Orthoptic screening consisted of cover tests, examination of eye motility and head posture, and monocular visual acuity testing with the Lea single optotype test. Children were re-examined in kindergarten by different orthoptists after 3-6 months using a more demanding pass threshold for visual acuity. All children with at least one positive orthoptic test result or an inconclusive re-examination were referred to an ophthalmologist for diagnosis. The gold standard was set positive if a target condition was diagnosed on ophthalmological examination. It was set negative if no target condition was found upon ophthalmological examination, or if a child who screened negative or inconclusive passed the orthoptic re-examination without any positive test result.
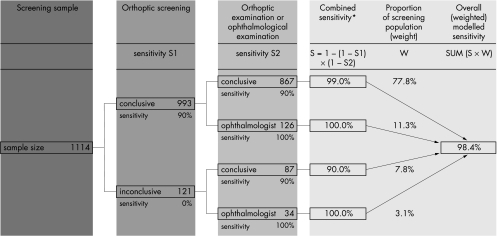
Results: The gold standard was ascertained in 1114 children. 26 (2.3%) children had a "positive" gold standard. In 10.8% of the children the initial screening was "inconclusive," mostly due to lack of collaboration. Screening test sensitivity (based on conclusive results only) was 90.9% and specificity was 93.8%.
Conclusions: Orthoptic vision screening of 3 year olds in kindergarten is sensitive and specific. However, owing to a substantial proportion of inconclusive screening results, rescreening of non-cooperative 3 year old children should be considered.
Figures
References
-
- Sjöstrand J, Abrahamsson M. Prevention of amblyopia and the concept of cure. Eur J Ophthalmol 1997;7:121–9. - PubMed
-
- Lennerstrand G, Jakobsson P, Kvarnström G. Screening for ocular dysfunction. Acta Ophthalmol Scand 1995;73(Suppl 214):26–38. - PubMed
-
- Fulton AB, Mayer DL. Esotropic children with amblyopia: effects of patching on acuity. Graefes Arch Clin Exp Ophthalmol 1988;226:309–12. - PubMed
-
- Egan DF, Brown R. Vision testing of young children in the age range of 18 months to 4½12 years. Child Care Health Dev 1984;10:381–90. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical