

Total occlusion versus hairline residual lumen of the internal carotid arteries: accuracy of single section helical CT angiography
- PMID: 12812937
- PMCID: PMC8149029
Total occlusion versus hairline residual lumen of the internal carotid arteries: accuracy of single section helical CT angiography
Abstract
Background and purpose: Routine carotid sonography and MR angiography cannot reliably detect the markedly reduced flow velocities associated with very severe carotid stenosis. In this study, we sought to evaluate the accuracy of single row detector helical CT angiography in distinguishing hairline residual lumen from total occlusion of severely stenosed internal carotid arteries (ICAs).
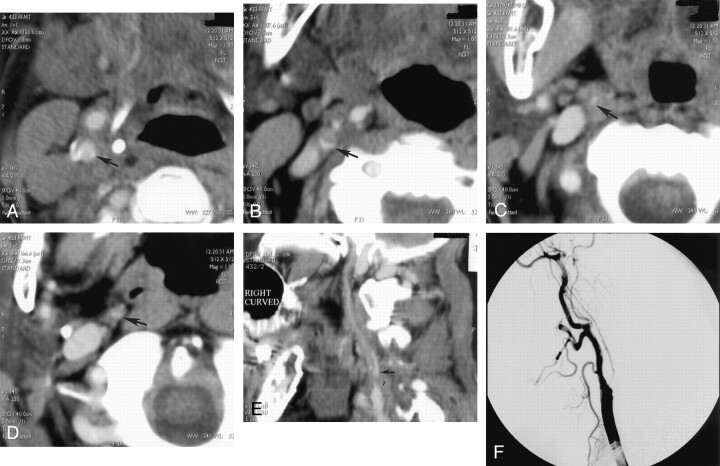
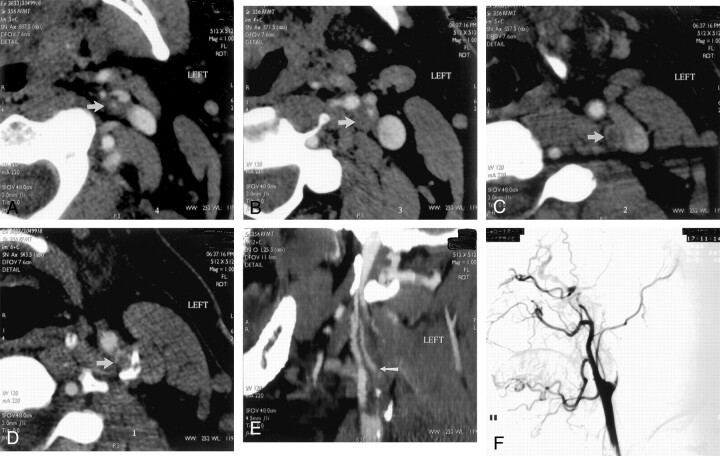
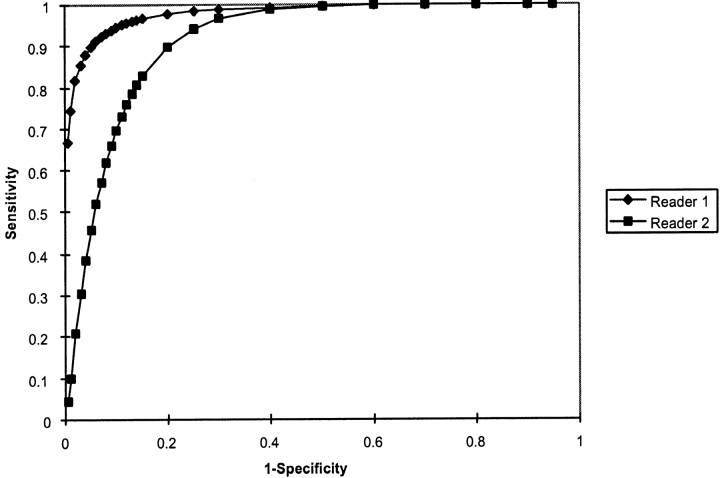
Methods: From our departmental data base of single row detector CT angiography studies performed for evaluation of ICA occlusive disease, 21 cases were identified with evidence of either hairline residual lumen or total occlusion on correlative conventional catheter radiographic arteriograms; these included seven cases of proved hairline residual lumen and 14 cases of proved total occlusion. Two neuroradiologists, blinded to the radiographic arteriography results, graded the diseased ICA on each CT angiogram as definitely occluded, probably occluded, indeterminate, probably patent, or definitely patent. Receiver operating characteristic curves were generated for each neuroradiologist.
Results: At an operating point on the receiver operating characteristic curve corresponding to 90% sensitivity, the first reader achieved 95% specificity and the second reader achieved 80% specificity for distinguishing hairline residual lumen from total occlusion. Absolute accuracy rates were 95% and 85%, respectively. No significant difference in accuracy was observed between the two readers (P =.28, two-tailed t test).
Conclusion: Single row detector CT angiography can distinguish total ICA occlusion from hairline residual lumen with a high degree of accuracy. In equivocal cases, conventional catheter arteriography may be desirable to confirm the diagnosis.
Figures
References
-
- Thiele BL, Young JV, Chikos PM, Hirsch JH, Strandness DE Jr. Correlation of arteriographic findings and symptoms in cerebrovascular disease. Neurology 1980;30:1041–1046 - PubMed
-
- North American Symptomatic Carotid Endarterectomy Trialists’ Collaborative Group. The final results of the NASCET trial. N Engl J Med 1998;339:1415–1425 - PubMed
-
- Lippman HH, Sundt TM Jr., Holman CB. The poststenotic carotid slim sign: supurious internal carotid hypolasia. Mayo Clin Proc 1970;45:762–767 - PubMed
-
- O’Leary DH, Mattle H, Potter JE. Atheromatous pseudo-occlusion of the internal carotid artery. Stroke 1989;20:1168–1173 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous