

Case Reports
Balloon-assisted coil placement in wide-neck bifurcation aneurysms by use of a new, compliant balloon microcatheter
Affiliations
- PMID: 12812958
- PMCID: PMC8149036
Item in Clipboard
Case Reports
Balloon-assisted coil placement in wide-neck bifurcation aneurysms by use of a new, compliant balloon microcatheter
AJNR Am J Neuroradiol.
2003 Jun-Jul.
Abstract
Two types of balloon are usually employed to perform balloon-assisted coil placement in cerebral aneurysms: oval, guide-dependent balloons for sidewall aneurysms and round balloons for bifurcation aneurysms. We report on the use of a new, more compliant, guide-dependent oval balloon microcatheter to seal wide-neck bifurcation aneurysms with coils during endovascular occlusion.
Figures
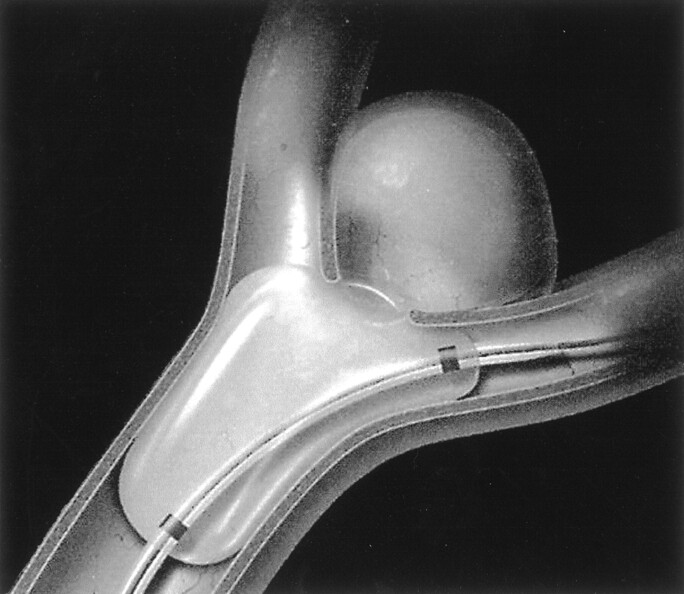
Sketch of the Hyperform balloon microcatheter illustrates sealing of the aneurysm neck and both bifurcated branches.
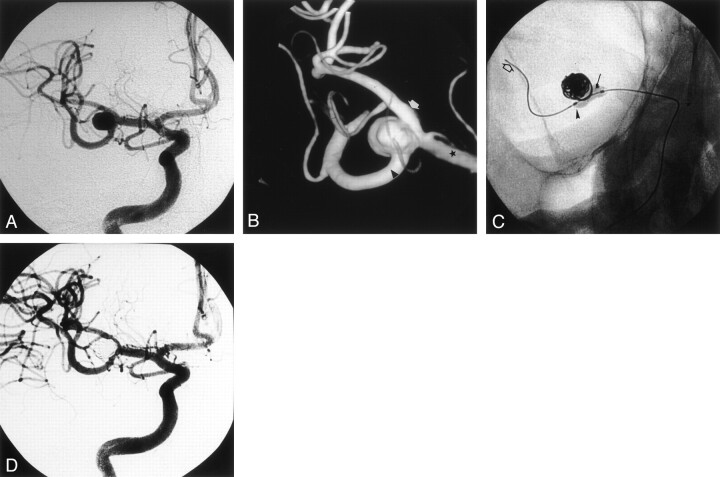
Case 1. A, Right internal carotid artery (ICA) angiogram, best projection, shows the MCA bifurcation aneurysm. B, Three-dimensional image of the right MCA bifurcation aneurysm shows the upper trunk (white arrow), the lower trunk (arrowhead), and the M1 segment (star) of the MCA. The lower trunk is clearly emerging from the neck of the aneurysm. C, Radiograph of the inflated Hyperform balloon into the MCA bifurcation. The balloon is bulging into the origin of the upper trunk (arrow), and its distal tip is positioned in the origin of the lower trunk (arrowhead). The Silver Speed (Silver Speed 10; Micro Therapeutics) guidewire is secured distally into the posterior temporal artery (open arrow). D, Right ICA control angiogram acquired at the end of the procedure shows total aneurysm occlusion and patency of upper and lower MCA trunks.
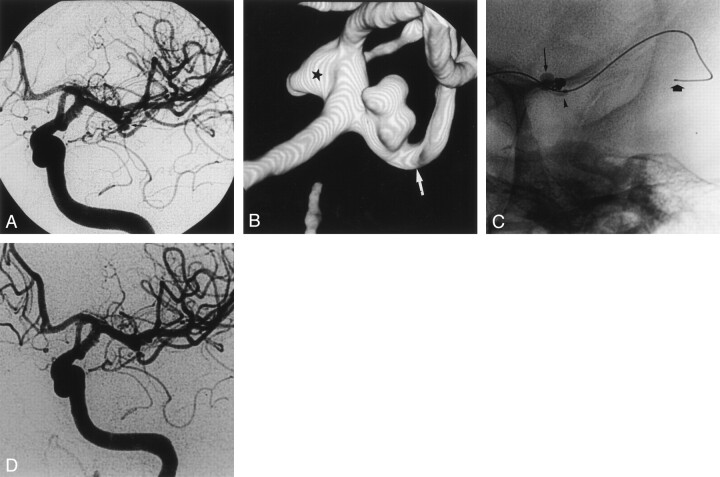
Case 2. A, Left ICA angiogram shows a bilobulated MCA bifurcation aneurysm (arrow). B, Three-dimensional angiogram shows the wide-neck aneurysm. The upper trunk origin appears dysplastic and enlarged (star). The lower trunk is indicated by the arrow. C, Radiograph of the inflated Hyperform balloon. The balloon bulges into the origin of the upper trunk (thin arrow), and its distal tip is positioned in the origin of the lower trunk (arrowhead). The Silver Speed guidewire is secured distally into the posterior temporal artery (thick arrow). D, Left ICA control angiogram acquired at the end of the procedure shows total aneurysm occlusion, with patency of both MCA upper and lower trunks.
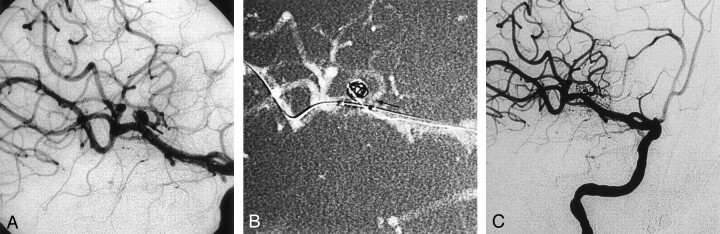
Case 3. A, Right ICA angiogram, best projection, shows the MCA aneurysm with the upper trunk (arrow) emerging from the sac. B, Right ICA angiogram, best projection, shows the Hyperform balloon inflated into the right MCA. The proximal part of the balloon is bulging into the origin of the upper trunk (arrow). C, Right ICA angiogram acquired at the end of the procedure shows that aneurysm occlusion is partial to preserve the patency of the upper trunk.
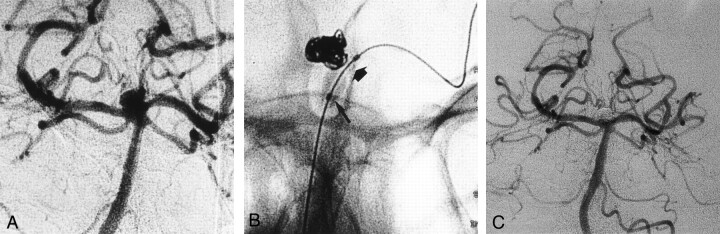
Case 4. A, Left vertebral angiogram, best frontal projection, shows the basilar tip aneurysm with unfavorable neck-to-fundus ratio. B, Radiograph of the inflated Hyperform balloon. The balloon is inflated across the neck. The distal part (thick arrow) of the Hyperform balloon is positioned into the left P1 segment, and its proximal part (thin arrow) is positioned into the basilar artery. The balloon conforms easily to both diameters of the basilar and the P1 segment of the left posterior cerebral artery. C, Left vertebral angiogram acquired after the procedure shows occlusion of the aneurysm with patency of both P1 segments.
References
-
- Moret J, Cognard C, Weill A, et al. [Reconstruction technic in the treatment of wide-neck intracranial aneurysms: long-term angiographic and clinical results apropos of 56 cases]. J Neuroradiol 1997;24:30–44 - PubMed
-
- Debrun GM, Aletich VA, Kehrli P, et al. Selection of cerebral aneurysms for treatment using Guglielmi detachable coils: the preliminary University of Illinois at Chicago experience. Neurosurgery 1998;43:1281–1295 - PubMed
-
- Mericle RA, Wakhloo AK, Rodriguez R, et al. Temporary balloon protection as an adjunct to endosaccular coiling of wide-necked cerebral aneurysms: technical note. Neurosurgery 1997;41:975–978 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical