

Hospital economics of the hospitalist
- PMID: 12822918
- PMCID: PMC1360922
- DOI: 10.1111/1475-6773.00152
Hospital economics of the hospitalist
Abstract
Objective: To determine the economic impact on the hospital of a hospitalist program and to develop insights into the relative economic importance of variables such as reductions in mean length of stay and cost, improvements in throughput (patients discharged per unit time), payer methods of reimbursement, and the cost of the hospitalist program.
Data sources: The primary data source was Tufts-New England Medical Center in Boston. Patient demographics, utilization, cost, and revenue data were obtained from the hospital's cost accounting system and medical records.
Study design: The hospitalist admitted and managed all patients during a six-week period on the general medical unit of Tufts-New England Medical Center. Reimbursement, cost, length of stay, and throughput outcomes during this period were contrasted with patients admitted to the unit in the same period in the prior year, in the preceding period, and in the following period.
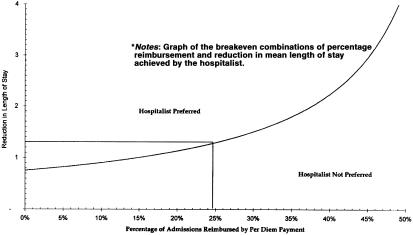
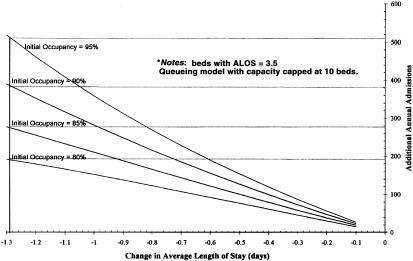
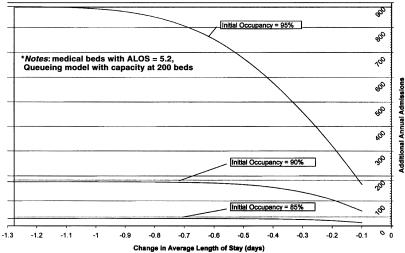
Principal findings: The hospitalist group compared with the control group demonstrated: length of stay reduced to 2.19 days from 3.45 days (p<.001); total hospital costs per admission reduced to 1,775 dollars from 2,332 dollars (p<.001); costs per day increased to 811 dollars from 679 dollars (p<.001); no differences for readmission within 30 days of discharge to extended care facilities. The hospital's expected incremental profitability with the hospitalist was -1.44 dollars per admission excluding incremental throughput effects, and it was most sensitive to changes in the ratio of per diem to case rate reimbursement. Incremental throughput with the hospitalist was estimated at 266 patients annually with an associated incremental profitability of 1.3 million dollars.
Conclusion: Hospital interventions designed to reduce length of stay, such as the hospitalist, should be evaluated in terms of cost, throughput, and reimbursement effects. Excluding throughput effects, the hospitalist program was not economically viable due to the influence of per diem reimbursement. Throughput improvements occasioned by the hospitalist program with high baseline occupancy levels are substantial and tend to favor a hospitalist program.
Figures
References
-
- American Hospital Association . Hospital Statistics. Chicago: American Hospital Association; 2001.
-
- Chen Q, Kane RL, Finch MD. “The Cost Effectiveness of Post-Acute Care for Elderly Medicare Beneficiaries.”. Inquiry. 2001;37:359–75. - PubMed
-
- Cunningham R. “Hospital Finance: Signs of ‘Pushback’ Amid Resurgent Cost Pressures.”. Health Affairs. 2001;20(2):234–340. - PubMed
-
- Diamond HS, Goldberg E, Janosky JE. “The Effect of Full-Time Hospitalists on the Efficiency of Care at a Community Teaching Hospital.”. Annals of Internal Medicine. 1998;129:197–203. - PubMed
-
- Freese RB. “The Park Nicollet Experience in Establishing a Hospitalist System.”. Annals of Internal Medicine. 1999;130:350–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
