

A strategy to reduce cardiovascular disease by more than 80%
- PMID: 12829553
- PMCID: PMC162259
- DOI: 10.1136/bmj.326.7404.1419
A strategy to reduce cardiovascular disease by more than 80%
Erratum in
- BMJ. 2003 Sep 13;327(7415):586
- BMJ. 2006 Sep;60(9):823
Abstract
Objectives: To determine the combination of drugs and vitamins, and their doses, for use in a single daily pill to achieve a large effect in preventing cardiovascular disease with minimal adverse effects. The strategy was to simultaneously reduce four cardiovascular risk factors (low density lipoprotein cholesterol, blood pressure, serum homocysteine, and platelet function) regardless of pretreatment levels.
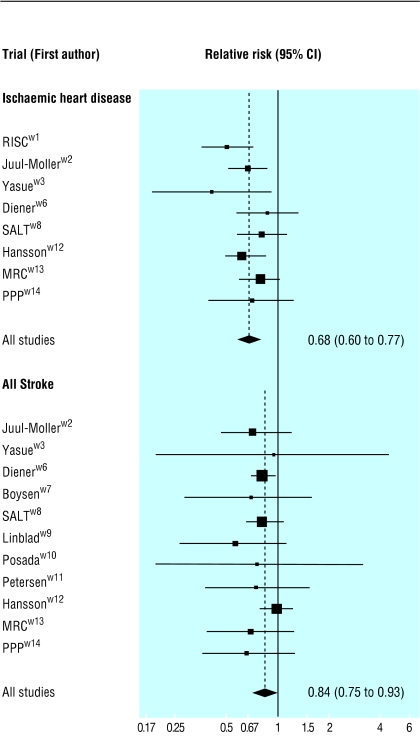
Design: We quantified the efficacy and adverse effects of the proposed formulation from published meta-analyses of randomised trials and cohort studies and a meta-analysis of 15 trials of low dose (50-125 mg/day) aspirin.
Outcome measures: Proportional reduction in ischaemic heart disease (IHD) events and strokes; life years gained; and prevalence of adverse effects.
Results: The formulation which met our objectives was: a statin (for example, atorvastatin (daily dose 10 mg) or simvastatin (40 mg)); three blood pressure lowering drugs (for example, a thiazide, a beta blocker, and an angiotensin converting enzyme inhibitor), each at half standard dose; folic acid (0.8 mg); and aspirin (75 mg). We estimate that the combination (which we call the Polypill) reduces IHD events by 88% (95% confidence interval 84% to 91%) and stroke by 80% (71% to 87%). One third of people taking this pill from age 55 would benefit, gaining on average about 11 years of life free from an IHD event or stroke. Summing the adverse effects of the components observed in randomised trials shows that the Polypill would cause symptoms in 8-15% of people (depending on the precise formulation).
Conclusion: The Polypill strategy could largely prevent heart attacks and stroke if taken by everyone aged 55 and older and everyone with existing cardiovascular disease. It would be acceptably safe and with widespread use would have a greater impact on the prevention of disease in the Western world than any other single intervention.
Figures

Comment in
-
A cure for cardiovascular disease? Combination treatment has enormous potential, especially in developing countries.BMJ. 2003 Jun 28;326(7404):1407-8. doi: 10.1136/bmj.326.7404.1407. BMJ. 2003. PMID: 12829526 Free PMC article. No abstract available.
-
"Polypill" to fight cardiovascular disease: now who's playing God?BMJ. 2003 Oct 4;327(7418):807; discussion 809; author reply 809-10. doi: 10.1136/bmj.327.7418.807-a. BMJ. 2003. PMID: 14525886 Free PMC article. No abstract available.
-
"Polypill" to fight cardiovascular disease: universal polypharmacy goes against recent beliefs in prescribing practice.BMJ. 2003 Oct 4;327(7418):807-8; discussion 809; author reply 809-10. doi: 10.1136/bmj.327.7418.807-b. BMJ. 2003. PMID: 14525887 Free PMC article. No abstract available.
-
"Polypill" to fight cardiovascular disease: patients before populations.BMJ. 2003 Oct 4;327(7418):807; discussion 809; author reply 809-10. doi: 10.1136/bmj.327.7418.807. BMJ. 2003. PMID: 14525888 Free PMC article. No abstract available.
-
"Polypill" to fight cardiovascular disease: cost effectiveness of statins for primary prevention of cardiovascular events is questionable.BMJ. 2003 Oct 4;327(7418):808-9; discussion 809; author reply 809-10. doi: 10.1136/bmj.327.7418.808-c. BMJ. 2003. PMID: 14525889 Free PMC article. No abstract available.
-
"Polypill" to fight cardiovascular disease: old joke has element of truth.BMJ. 2003 Oct 4;327(7418):808; discussion 809; author reply 809-10. doi: 10.1136/bmj.327.7418.808. BMJ. 2003. PMID: 14525890 Free PMC article. No abstract available.
-
"Polypill" to fight cardiovascular disease: interpretation of trial data is optimistic.BMJ. 2003 Oct 4;327(7418):808; discussion 809; author reply 809-10. doi: 10.1136/bmj.327.7418.808-b. BMJ. 2003. PMID: 14525891 Free PMC article. No abstract available.
-
"Polypill" to fight cardiovascular disease: birthday present was much appreciated.BMJ. 2003 Oct 4;327(7418):808; discussion 809; author reply 809-10. doi: 10.1136/bmj.327.7418.808-a. BMJ. 2003. PMID: 14525892 Free PMC article. No abstract available.
-
Polypill debate continues: people will always be sceptical.BMJ. 2004 Jan 31;328(7434):289. doi: 10.1136/bmj.328.7434.289-b. BMJ. 2004. PMID: 14751916 Free PMC article. No abstract available.
-
Revalidation: swallow hard.BMJ. 2004 May 1;328(7447):1077. doi: 10.1136/bmj.328.7447.1077-a. BMJ. 2004. PMID: 15117807 Free PMC article. No abstract available.
References
-
- MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, Neaton J, et al. Blood pressure, stroke and coronary heart disease. Part 1: prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 1990;335: 765-74. - PubMed
-
- Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA, et al. Blood pressure, stroke and coronary heart disease. Part 2: short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet 1990;335: 827-38 - PubMed
-
- Law MR, Wald NJ, Morris JK. Lowering blood pressure to prevent myocardial infarction and stroke: a new prevention strategy. Health Technol Assess (in press). - PubMed
-
- PATS Collaborating Group. Post-stroke antihypertensive treatment study. Chin Med J 1995;108: 710-17. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous