

Antral hyperplastic polyp causing intermittent gastric outlet obstruction: case report
- PMID: 12831404
- PMCID: PMC166166
- DOI: 10.1186/1471-230X-3-16
Antral hyperplastic polyp causing intermittent gastric outlet obstruction: case report
Abstract
Background: Hyperplastic polyps are the most common polypoid lesions of the stomach. Rarely, they cause gastric outlet obstruction by prolapsing through the pyloric channel, when they arise in the prepyloric antrum.
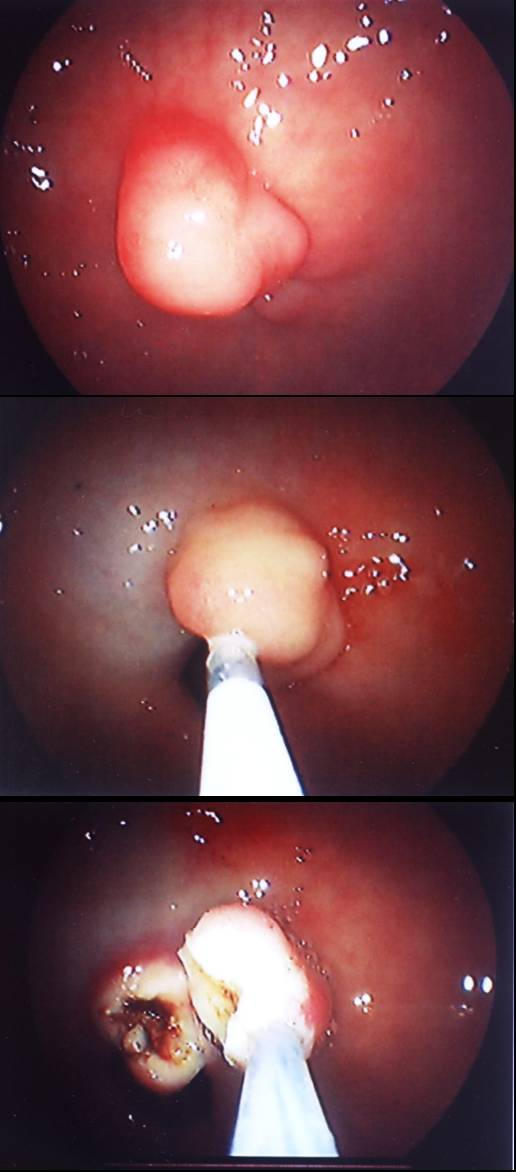
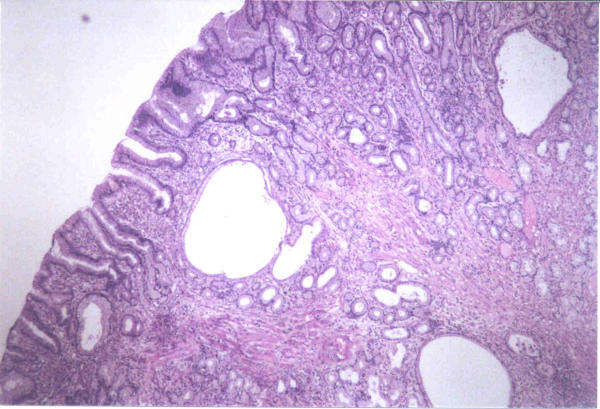
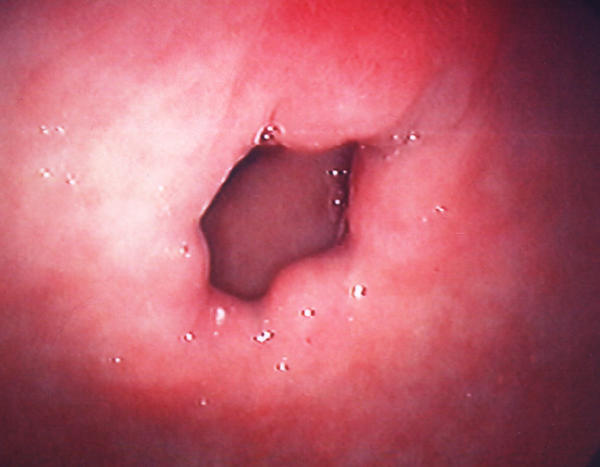
Case presentation: A 62-year-old woman presented with intermittent nausea and vomiting of 4 months duration. Upper gastrointestinal endoscopy revealed a 30 mm prepyloric sessile polyp causing intermittent gastric outlet obstruction. Following submucosal injection of diluted adrenaline solution, the polyp was removed with a snare. Multiple biopsies were taken from the greater curvature of the antrum and the corpus. Rapid urease test for Helicobacter pylori yielded a negative result. Histopathologic examination showed a hyperplastic polyp without any evidence of malignancy. Biopsies of the antrum and the corpus revealed gastritis with neither atrophic changes nor Helicobacter pylori infection. Follow-up endoscopy after a 12-week course of proton pomp inhibitor therapy showed a complete healing without any remnant tissue at the polypectomy site. The patient has been symptom-free during 8 months of follow-up.
Conclusions: Symptomatic gastric polyps should be removed preferentially when they are detected at the initial diagnostic endoscopy. Polypectomy not only provides tissue to determine the exact histopathologic type of the polyp, but also achieves radical treatment.
Figures
Similar articles
-
Endoscopic management of multiple large antral hyperplastic polyps causing gastric outlet obstruction.Ann Ital Chir. 2011 Jul-Aug;82(4):297-300. Ann Ital Chir. 2011. PMID: 21834480
-
Pyloric obstruction caused by prolapse of a hyperplastic gastric polyp.Hepatogastroenterology. 2002 Jul-Aug;49(46):958-60. Hepatogastroenterology. 2002. PMID: 12143253
-
Prolapsing Gastric Polyp Causing Intermittent Gastric Outlet Obstruction.Int Surg. 2015 Jun;100(6):1148-52. doi: 10.9738/INTSURG-D-14-00205.1. Epub 2015 Jan 11. Int Surg. 2015. PMID: 25578789 Free PMC article.
-
Benign intermittent gastric outlet obstruction in an elderly: endoscopic management and brief review.Niger J Med. 2010 Oct-Dec;19(4):479-81. doi: 10.4314/njm.v19i4.61981. Niger J Med. 2010. PMID: 21526644 Review.
-
Hyperplastic gastric polyp causing progressive gastric outlet obstruction.Mayo Clin Proc. 1998 Oct;73(10):964-7. doi: 10.4065/73.10.964. Mayo Clin Proc. 1998. PMID: 9787747 Review.
Cited by
-
Endoscopic Removal of a Giant Complicated Hyperplastic Gastric Polyp.Open Access Maced J Med Sci. 2017 Oct 16;5(7):1047-1048. doi: 10.3889/oamjms.2017.188. eCollection 2017 Dec 15. Open Access Maced J Med Sci. 2017. PMID: 29362643 Free PMC article.
-
Minute signet ring cell carcinoma occurring in gastric hyperplastic polyp.World J Gastroenterol. 2007 Nov 21;13(43):5779-80. doi: 10.3748/wjg.v13.i43.5779. World J Gastroenterol. 2007. PMID: 17963309 Free PMC article.
-
Endoscopic Management of Gastric Polyp with Outlet Obstruction without Polypectomy.Case Rep Gastroenterol. 2011 May;5(2):267-71. doi: 10.1159/000328443. Epub 2011 May 3. Case Rep Gastroenterol. 2011. PMID: 21887127 Free PMC article.
-
Gastric hyperplastic polyps: a review.Dig Dis Sci. 2009 Sep;54(9):1839-46. doi: 10.1007/s10620-008-0572-8. Epub 2008 Nov 27. Dig Dis Sci. 2009. PMID: 19037727 Review.
-
Antral hyperplastic polyp: A rare cause of gastric outlet obstruction.Int J Surg Case Rep. 2014;5(6):287-9. doi: 10.1016/j.ijscr.2014.03.016. Epub 2014 Mar 25. Int J Surg Case Rep. 2014. PMID: 24747755 Free PMC article.
References
-
- Livingston EH. Stomach and duodenum. In: Norton JA, Bollinger RR, Chang AE, Lowry SF, Mulvihill SJ, Pass HI, Thompson RW, editor. In Surgery: Basic Science and Clinical Evidence. New York: Springer-Verlag; 2000. pp. 489–515.
-
- Gencosmanoglu R, Sad O, Sav A, Tozun N. Primary hypertrophic pyloric stenosis in the adult: a case report. Turkish J Gastroenterol. 2002;13:175–179. - PubMed
-
- Dean PG, Davis PM, Nascimento AG, Farley DR. Hyperplastic gastric polyp causing progressive gastric outlet obstruction. Mayo Clin Proc. 1998;73:964–967. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
