

Results of surgical resection for patients with hilar bile duct cancer: application of extended hepatectomy after biliary drainage and hemihepatic portal vein embolization
- PMID: 12832969
- PMCID: PMC1422661
- DOI: 10.1097/01.SLA.0000074984.83031.02
Results of surgical resection for patients with hilar bile duct cancer: application of extended hepatectomy after biliary drainage and hemihepatic portal vein embolization
Abstract
Objective: To evaluate the feasibility of an aggressive surgical approach incorporating major hepatic resection after biliary drainage and preoperative portal vein embolization for patients with hilar bile duct cancer.
Summary background data: Although many surgeons have emphasized the importance of major hepatectomy in terms of curative resection for patients with hilar bile duct cancer, this procedure results in a high incidence of postoperative morbidity and mortality in patients with cholestasis-induced impaired liver function.
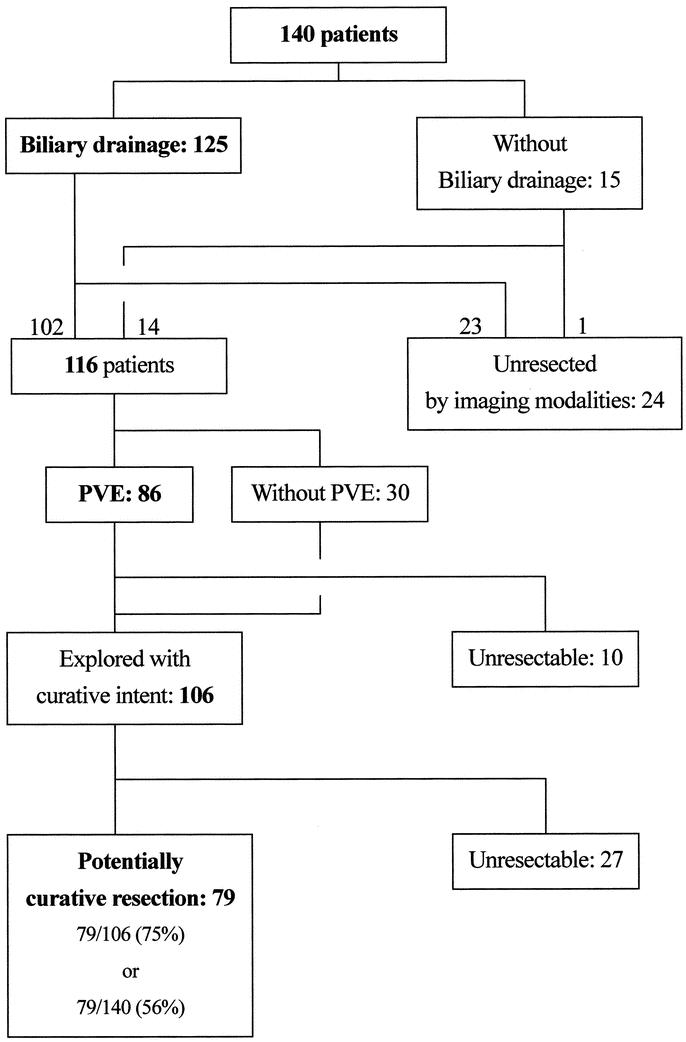
Methods: A retrospective cohort study was conducted in 140 patients with hilar bile duct cancer treated from 1990 through 2001. Resectional surgery was performed in 79 patients, 69 of whom underwent major hepatic resection. Thirteen patients underwent concomitant pancreaticoduodenectomy. Preoperative biliary drainage was carried out in all 65 patients who had obstructive jaundice. Portal vein embolization was conducted in 41 of 51 patients undergoing extended right hepatectomy. Short- and long-term outcomes were evaluated.
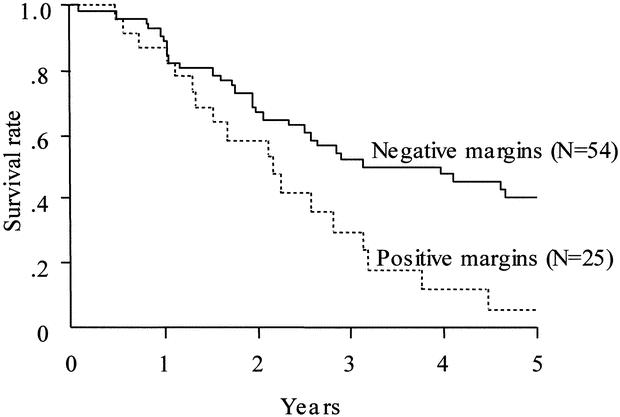
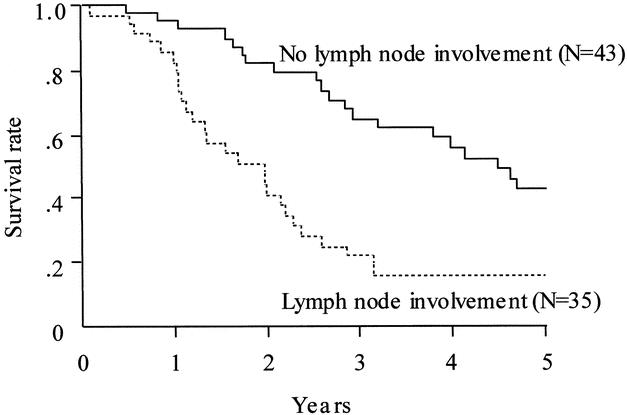
Results: No patient experienced postoperative liver failure (maximum total bilirubin level, 5.4 mg/dL). The in-hospital mortality rate was 1.3% (1 in 79, resulting from cerebral infarction). A histologically negative resection margin was obtained more frequently when the scheduled extended hepatic resection was conducted (75% vs 44%, P = 0.0178). The estimated 5-year survival rate was 40% when histologically negative resection margins were obtained, but only 6% if the margins were positive. Multivariate analysis identified the resection margin and nodal status as independent factors predictive of survival.
Conclusions: Extensive resection, mainly extended right hemihepatectomy, after biliary drainage and preoperative portal vein embolization, when necessary, for patients with hilar bile duct cancer can be performed safely and is more likely to result in histologically negative margins than other resection methods.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
