

Allelic imbalance at chromosome 11 in head and neck squamous cell carcinoma in an Indian patient population
- PMID: 12835296
- PMCID: PMC1769990
- DOI: 10.1136/jcp.56.7.512
Allelic imbalance at chromosome 11 in head and neck squamous cell carcinoma in an Indian patient population
Abstract
Background: Genetic instability of chromosome 11 is a frequent event in many solid tumours, including head and neck squamous cell carcinoma (HNSCC).
Aims: To perform allelic imbalance analysis of cytogenetically mapped altered regions of human chromosome 11 in patients with HNSCC from eastern India.
Methods: Genomic alterations were investigated using highly polymorphic microsatellite markers in both HNSCC and leukoplakia tissues.
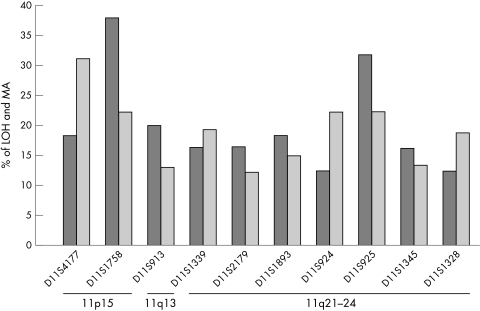
Results: Microsatellite markers D11S1758 from 11p13-15 and D11S925 from 11q23.3-24 had the highest frequency (38% and 32%, respectively) of loss of heterozygosity among all the markers analysed. Allelic loss at the marker D11S925 was seen in both leukoplakia and in all stages of HNSCC tumour tissues suggesting that it is an early event in HNSCC tumorigenesis. Microsatellite size alteration was also found to be high (> 20%) in several markers. In leukoplakia samples microsatellite instability was seen at a higher frequency than loss of the allele, indicating such alterations might initiate the process of tumorigenesis in HNSCC.
Conclusions: The high rate of chromosomal alterations at 11q21-24 in HNSCC suggests the presence of a putative tumour suppressor gene in this region.
Figures





References
-
- Parkin DM, Pisani P, Ferlay J, et al. Estimates of the worldwide incidence of eighteen major cancers in 1985. Int J Cancer 1993;54:594–600. - PubMed
-
- Saranath D, Bhoite LT, Deo MG, et al. Molecular lesion in human oral cancer: the Indian scene, oral oncology. Eur J Cancer 1993;29:107–12. - PubMed
-
- Wu CL, Solan P, Thakker N, et al. Deletion mapping on the short arm of chromosome 3 in squamous cell carcinoma of the oral cavity. Cancer Res 1994;54:6484–8. - PubMed
-
- Van Dyke D, Worsham MJ, Beninger MS, et al. Recurrent cytogenetic abnormalities in squamous cell carcinomas of the head and neck region. Genes Chromosomes Cancer 1994;9:192–206. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical