

Study of viral integration of HPV-16 in young patients with LSIL
- PMID: 12835300
- PMCID: PMC1770000
- DOI: 10.1136/jcp.56.7.532
Study of viral integration of HPV-16 in young patients with LSIL
Abstract
Aims: To investigate the physical status of human papillomavirus 16 (HPV-16) in low grade squamous intraepithelial lesions (LSILs) as a means of determining the percentage of viral integration.
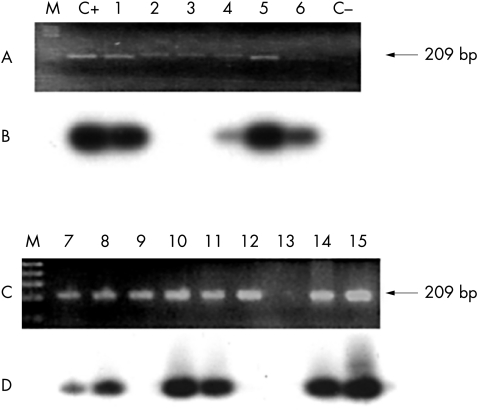
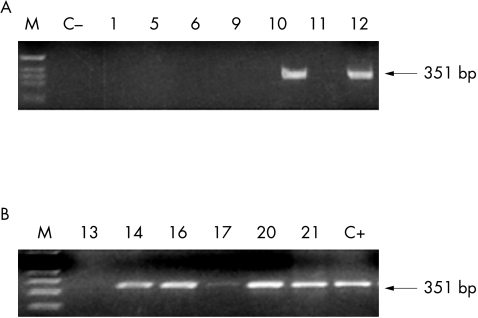
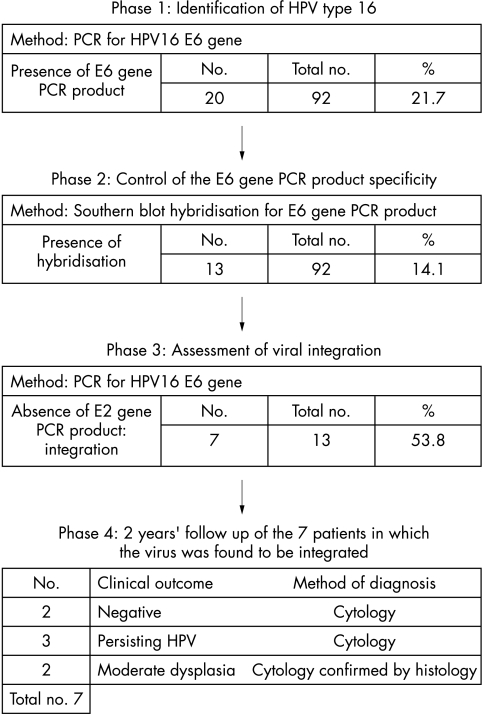
Methods: Ninety two LSIL/HPV positive Thin Prep(TM) samples were initially tested for the E6 gene by the polymerase chain reaction (PCR) to identify the HPV-16 virus. To avoid false positive results, the specificity of the bands obtained from PCR was confirmed by Southern blot hybridisation with internal oligonucleotide probes. Next, a PCR screen for the E2 gene was performed to identify those samples in which the virus was integrated. Viral integration was detected in just over half of them.
Results: Twenty of the 92 samples were HPV-16 positive, as shown by PCR for the E6 gene. Southern blot analysis confirmed that 13 of these samples were positive for the viral E6 gene. Thus, viral integration was detected in just over a half of the samples positive for HPV-16.
Conclusions: These data show that HPV-16 integration occurs in a subset of LSILs. The measurement of HPV-16 integration would be a helpful complementary tool for cytological evaluation in primary cervical screening to identify those patients at risk of developing high grade squamous intraepithelial lesions and cervical cancer.
Figures
References
-
- Zwerschke W, Jansen-Dürr P. Cell transformation by the E7 oncoprotein of human papillomavirus type 16: interactions with nuclear and cytoplasmic target proteins. Adv Cancer Res 2000;78:1–29. - PubMed
-
- Arends MJ, Wyllie AH, Bird CC. Papillomaviruses and human cancer. Hum Pathol 1990;21:686–98. - PubMed
-
- Arends MJ, Donaldson YK, Duvall E, et al. HPV in full thickness cervical biopsies: high prevalence in CIN 2 and CIN 3 detected by a sensitive PCR method. J Pathol 1991;165:301–9. - PubMed
-
- Arends MJ, Donaldson YK, Duvall E, et al. HPV 18 associates with a more advanced cervical neoplasia than HPV 16. Hum Pathol 1993;24:432–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous