

Surgeon specific mortality in adult cardiac surgery: comparison between crude and risk stratified data
- PMID: 12842949
- PMCID: PMC164230
- DOI: 10.1136/bmj.327.7405.13
Surgeon specific mortality in adult cardiac surgery: comparison between crude and risk stratified data
Abstract
Objective: As a result of recent failures in clinical governance the government has made a commitment to bring individual surgeons' mortality data into the public domain. We have analysed a database to compare crude mortality after coronary artery bypass surgery with outcomes that were stratified by risk.
Design: Retrospective analysis of prospectively collected data.
Setting: All NHS centres in the geographical north west of England that undertake cardiac surgery in adults.
Participants: All patients undergoing isolated bypass graft surgery for the first time between April 1999 and March 2002.
Main outcome measures: Surgeon specific postoperative mortality and predicted mortality by EuroSCORE.
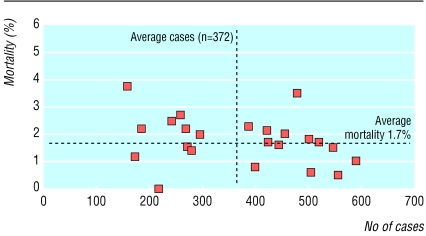
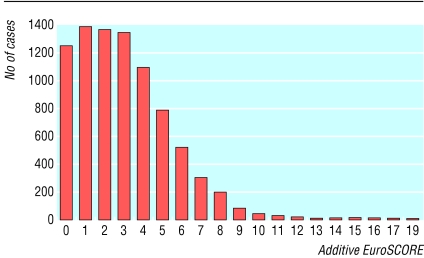
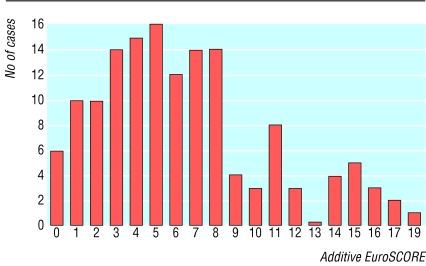
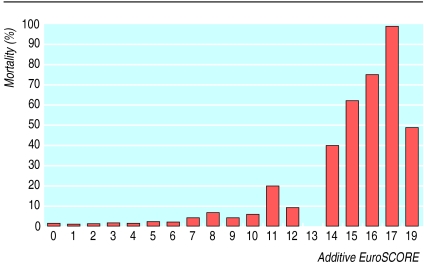
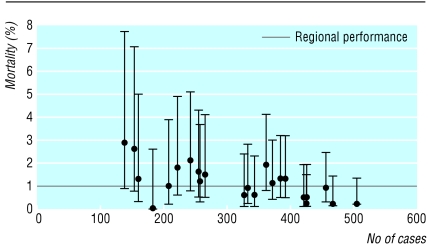
Results: 8572 patients were operated on by 23 surgeons. Overall mortality was 1.7%. Observed mortality between surgeons ranged from 0% to 3.7%; predicted mortality ranged from 2% to 3.7%. Eighty five per cent (7286) of the patients had a EuroSCORE of 5 or less; 49% of the deaths were in this lower risk group. A large proportion of the variability in predicted mortality between surgeons was due to a small but differing number of high risk patients.
Conclusions: It is possible to collect risk stratified data on all patients undergoing coronary bypass surgery. For most the predicted mortality is low. The small proportion of high risk patients is responsible for most of the differences in predicted mortality between surgeons. Crude comparisons of death rates can be misleading and may encourage surgeons to practise risk averse behaviour. We recommend a comparison of death rates that is stratified by risk and based on low risk cases as the national benchmark for assessing consultant specific performance.
Figures
Comment in
-
Surgeon specific mortality in adult cardiac surgery: higher risk cases need also to be assessed.BMJ. 2003 Sep 6;327(7414):563. doi: 10.1136/bmj.327.7414.563-c. BMJ. 2003. PMID: 12958126 Free PMC article. No abstract available.
-
Surgeon specific mortality in adult cardiac surgery: quality of data is important.BMJ. 2003 Sep 6;327(7414):563. doi: 10.1136/bmj.327.7414.563-b. BMJ. 2003. PMID: 12958128 Free PMC article. No abstract available.
References
-
- Keogh B, Kinsman R. National adult cardiac surgical database report 2000-2001. London: Society of Cardiothoracic Surgeon of Great Britain and Ireland, 2002.
-
- Parsonnet V, Dean D, Bernstein AD. A method of uniform stratification of risk for evaluating the results of surgery in acquired heart disease. Circulation 1979;I3- I12. - PubMed
-
- Tu JV, Jaglal SB, Naylor D. Multicenter validation of a risk index for mortality, intensive care unit stay, and overall hospital length of stay after cardiac surgery. Circulation 1995;91: 677-84. - PubMed
-
- Roques F, Nashef SA, Michel P, Guaducheau E, de Vincentiis C, Baudet E, et al. Risk factors and outcome in European cardiac surgery; analysis of the EuroSCORE multinational database of 19,030 patients. Eur J Cardiothorac Surg 1999;15: 816-23. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous