

Prospective observational cohort study of time saved by prehospital thrombolysis for ST elevation myocardial infarction delivered by paramedics
- PMID: 12842951
- PMCID: PMC164234
- DOI: 10.1136/bmj.327.7405.22
Prospective observational cohort study of time saved by prehospital thrombolysis for ST elevation myocardial infarction delivered by paramedics
Abstract
Objectives: To evaluate a system of prehospital thrombolysis, delivered by paramedics, in meeting the national service framework's targets for the management of acute myocardial infarction.
Design: Prospective observational cohort study comparing patients with suspected acute myocardial infarction considered for thrombolysis in the prehospital environment with patients treated in hospital.
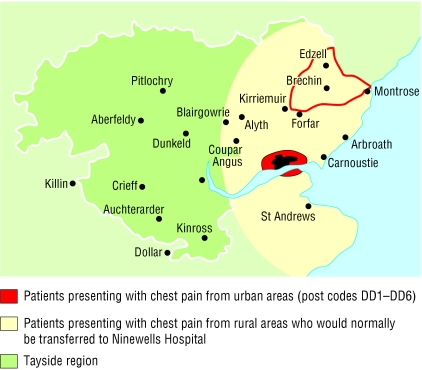
Setting: The catchment area of a large teaching hospital, including urban and rural areas.
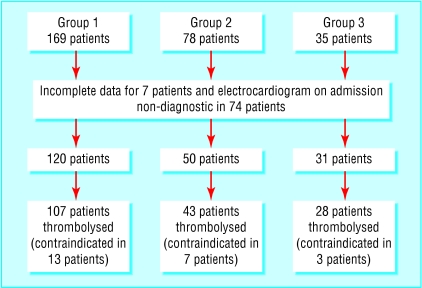
Participants: 201 patients presenting concurrently over a 12 month period who had changes to the electrocardiogram that were diagnostic of acute myocardial infarction or who received thrombolysis for suspected acute myocardial infarction.
Main outcome measures: Time from first medical contact to initiation of thrombolysis (call to needle time), number of patients given thrombolysis appropriately, and all cause mortality in hospital.
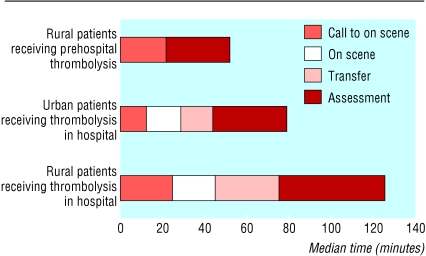
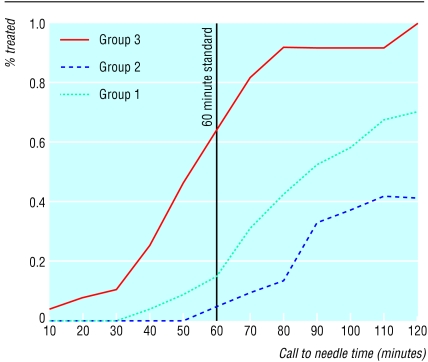
Results: The median call to needle time for patients treated before arriving in hospital (n=28) was 52 (95% confidence interval 41 to 62) minutes. Patients from similar rural areas who were treated in hospital (n=43) had a median time of 125 (104 to 140) minutes. This represents a median time saved of 73 minutes (P < 0.001). Sixty minutes after medical contact 64% of patients (18/28) treated before arrival in hospital had received thrombolysis; this compares with 4% of patients (2/43) in a cohort from similar areas. Median call to needle time for patients from urban areas (n=107) was 80 (78 to 93) minutes. Myocardial infarction was confirmed in 89% of patients (25/28) who had received prehospital thrombolysis; this compares with 92% (138/150) in the two groups of patients receiving thrombolysis in hospital.
Conclusions: Thrombolysis delivered by paramedics with support from the base hospital can meet the national targets for early thrombolysis. The system has been shown to work well and can be introduced without delay.
Figures
Comment in
-
Prehospital thrombolysis.BMJ. 2003 Jul 5;327(7405):1-2. doi: 10.1136/bmj.327.7405.1. BMJ. 2003. PMID: 12842922 Free PMC article. No abstract available.
-
Costs and effectiveness of prehospital thrombolysis need to be clear.BMJ. 2003 Nov 1;327(7422):1051. doi: 10.1136/bmj.327.7422.1051-a. BMJ. 2003. PMID: 14593065 Free PMC article. No abstract available.
Similar articles
-
Retrospective observational case-control study comparing prehospital thrombolytic therapy for ST-elevation myocardial infarction with in-hospital thrombolytic therapy for patients from same area.Emerg Med J. 2005 Aug;22(8):582-5. doi: 10.1136/emj.2004.020271. Emerg Med J. 2005. PMID: 16046765 Free PMC article.
-
Factors influencing the time to thrombolysis in acute myocardial infarction. Time to Thrombolysis Substudy of the National Registry of Myocardial Infarction-1.Arch Intern Med. 1997 Dec 8-22;157(22):2577-82. Arch Intern Med. 1997. PMID: 9531226
-
Prehospital management of acute myocardial infarction: Electrocardiogram acquisition and interpretation, and thrombolysis by prehospital care providers.Can J Cardiol. 1998 Oct;14(10):1231-40. Can J Cardiol. 1998. PMID: 9852937 Review.
-
Management of prehospital thrombolytic therapy in ST-segment elevation acute coronary syndrome (<12 hours).Minerva Anestesiol. 2005 Jun;71(6):297-302. Minerva Anestesiol. 2005. PMID: 15886591 Review.
-
Pre-hospital thrombolysis delivered by paramedics is associated with reduced time delay and mortality in ambulance-transported real-life patients with ST-elevation myocardial infarction.Eur Heart J. 2006 May;27(10):1146-52. doi: 10.1093/eurheartj/ehi886. Epub 2006 Apr 19. Eur Heart J. 2006. PMID: 16624832
Cited by
-
Thrombolytic therapy for myocardial infarction facilitated by mobile coronary care.Ulster Med J. 2004 Nov;73(2):77-84. Ulster Med J. 2004. PMID: 15651765 Free PMC article.
-
Clinical Research in Prehospital Care: Current and Future Challenges.Clin Pract. 2023 Oct 23;13(5):1266-1285. doi: 10.3390/clinpract13050114. Clin Pract. 2023. PMID: 37887090 Free PMC article. Review.
-
Primary Angioplasty for the Treatment of Acute ST-Segment Elevated Myocardial Infarction: An Evidence-Based Analysis.Ont Health Technol Assess Ser. 2004;4(10):1-65. Epub 2004 Aug 1. Ont Health Technol Assess Ser. 2004. PMID: 23074449 Free PMC article.
-
Prehospital thrombolysis--calculated health benefit for catchment population of one hospital.J R Soc Med. 2004 May;97(5):230-4. doi: 10.1177/014107680409700506. J R Soc Med. 2004. PMID: 15121813 Free PMC article.
-
Emergency department thrombolysis improves door to needle times.Emerg Med J. 2004 Nov;21(6):676-80. doi: 10.1136/emj.2004.014449. Emerg Med J. 2004. PMID: 15496692 Free PMC article.
References
-
- Fibrinolytic Therapy Triallists' (FTT) Collaborative Group. Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Lancet 1994;343: 311-22. - PubMed
-
- Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. Lancet 1988; 332: 349-60. - PubMed
-
- Boersma E, Maas ACP, Deckers JW, Simoons ML. Early thrombolytic treatment in acute myocardial infarction: reappraisal of the golden hour. Lancet 1996;348: 771-5. - PubMed
-
- Morrison LJ, Verbeek PR, McDonald AC, Sawadsky BV, Cook DJ. Mortality and prehospital thrombolysis for acute myocardial infarction. A meta-analysis. JAMA 2000;283: 2686-92. - PubMed
-
- Department of Health. National service framework for coronary heart disease. London: DoH, 2000. www.doh.gov.uk/nsf/coronary.htm (accessed 6 Jun 2003).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous