

The clinical pathology of severe acute respiratory syndrome (SARS): a report from China
- PMID: 12845623
- PMCID: PMC7168017
- DOI: 10.1002/path.1440
The clinical pathology of severe acute respiratory syndrome (SARS): a report from China
Abstract
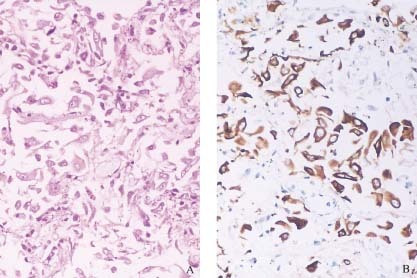
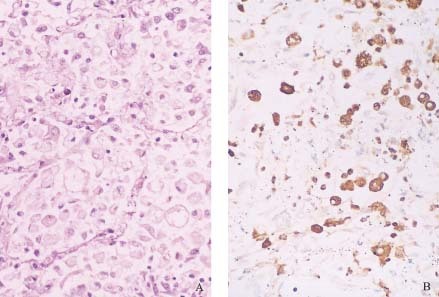
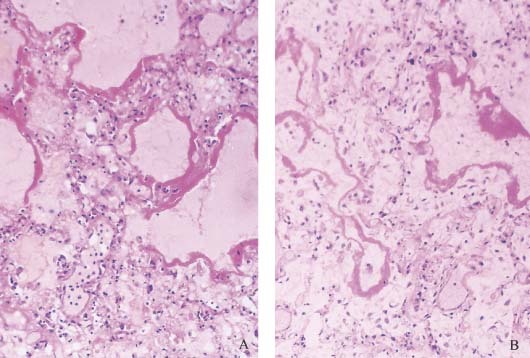
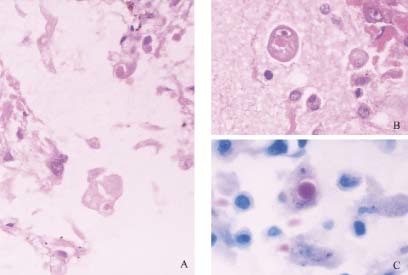
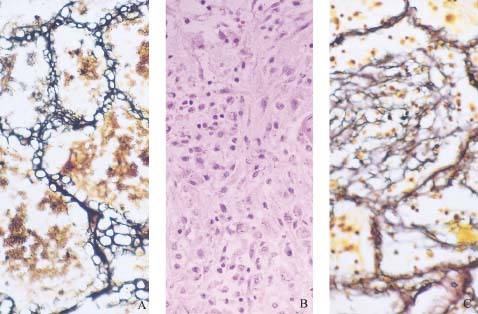
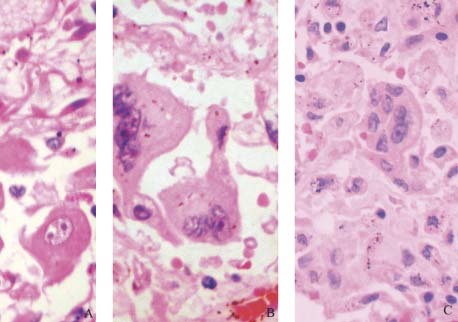
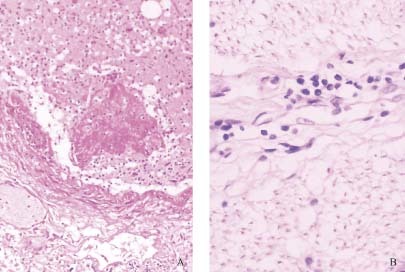
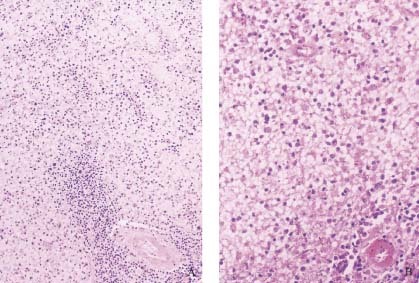
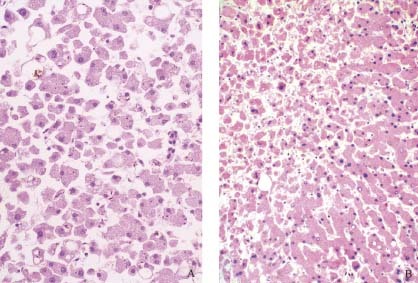
In order to investigate the clinical pathology of severe acute respiratory syndrome (SARS), the autopsies of three patients who died from SARS in Nan Fang Hospital Guangdong, China were studied retrospectively. Routine haematoxylin and eosin (H&E) staining was used to study all of the tissues from the three cases. The lung tissue specimens were studied further with Macchiavello staining, viral inclusion body staining, reticulin staining, PAS staining, immunohistochemistry, ultrathin sectioning and staining, light microscopy, and transmission electron microscopy. The first symptom was hyperpyrexia in all three cases, followed by progressive dyspnoea and lung field shadowing. The pulmonary lesions included bilateral extensive consolidation, localized haemorrhage and necrosis, desquamative pulmonary alveolitis and bronchitis, proliferation and desquamation of alveolar epithelial cells, exudation of protein and monocytes, lymphocytes and plasma cells in alveoli, hyaline membrane formation, and viral inclusion bodies in alveolar epithelial cells. There was also massive necrosis of splenic lymphoid tissue and localized necrosis in lymph nodes. Systemic vasculitis included oedema, localized fibrinoid necrosis, and infiltration of monocytes, lymphocytes, and plasma cells into vessel walls in the heart, lung, liver, kidney, adrenal gland, and the stroma of striated muscles. Thrombosis was present in small veins. Systemic toxic changes included degeneration and necrosis of the parenchyma cells in the lung, liver, kidney, heart, and adrenal gland. Electron microscopy demonstrated clusters of viral particles, consistent with coronavirus, in lung tissue. SARS is a systemic disease that injures many organs. The lungs, immune organs, and systemic small vessels are the main targets of virus attack, so that extensive consolidation of the lung, diffuse alveolar damage with hyaline membrane formation, respiratory distress, and decreased immune function are the main causes of death.
Copyright 2003 John Wiley & Sons, Ltd.
Figures


References
-
- Update: Outbreak of severe acute respiratory syndrome‐worldwide. Morb Mortal Wkly Rep 2003; 52(11): 241–248. - PubMed
-
- Tsang KW, Ho PL, Ooi GC, et al. A cluster of cases of severe acute respiratory syndrome in Hong Kong. N Engl J Med 2003; 348: 1–9 (published at http://www.nejm.org. [31 March 2003]). - PubMed
-
- Poutanen SM, Low DE, Henry B, et al. Identification of severe acute respiratory syndrome in Canada. N Engl J Med 2003; 348: 1–11 (published at http://www.nejm.org. [31 March 2003]). - PubMed
-
- Thomas G, Ksiazek D, Erdman D, et al. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med 2003; 348(20): 1953–1966. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
