

A randomized controlled trial of a pharmacist consultation program for family physicians and their elderly patients
- PMID: 12847034
- PMCID: PMC164937
A randomized controlled trial of a pharmacist consultation program for family physicians and their elderly patients
Abstract
Background: Pharmacists can improve patient outcomes in institutional and pharmacy settings, but little is known about their effectiveness as consultants to primary care physicians. We examined whether an intervention by a specially trained pharmacist could reduce the number of daily medication units taken by elderly patients, as well as costs and health care use.
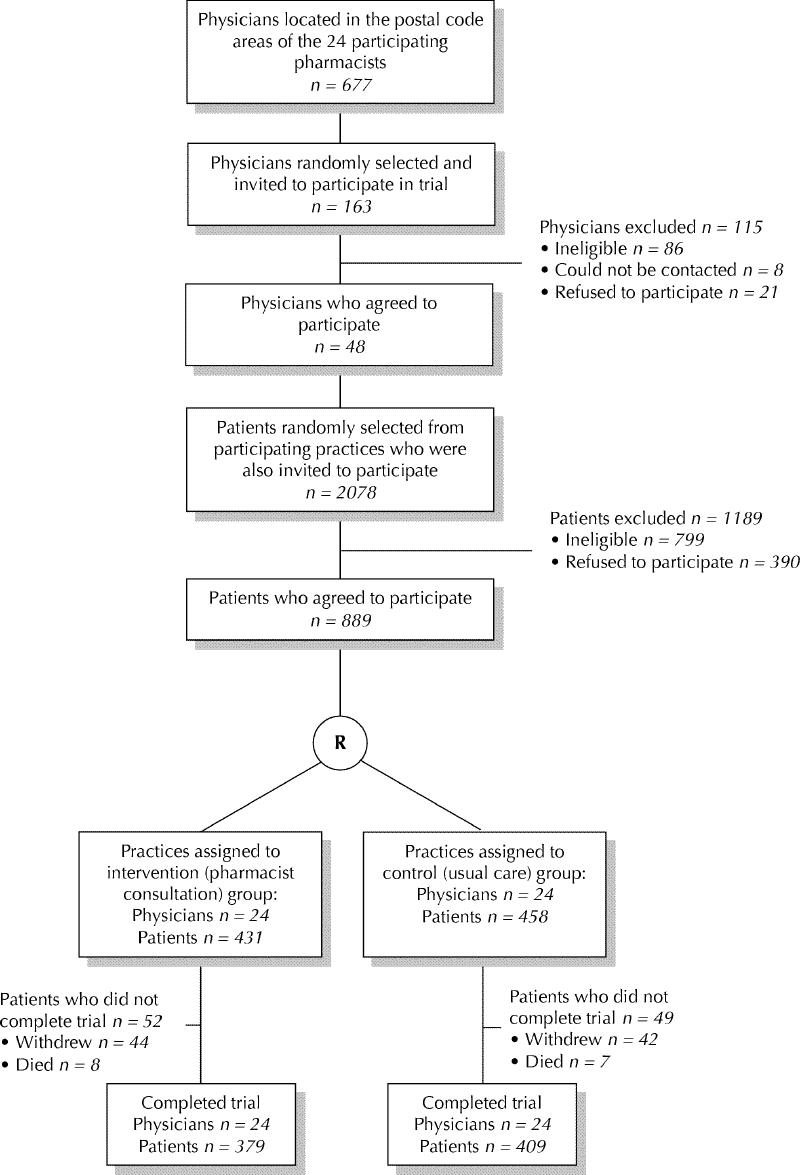
Methods: We conducted a randomized controlled trial in family practices in 24 sites in Ontario. We randomly allocated 48 randomly selected family physicians (69.6% participation rate) to the intervention or the control arm, along with 889 (69.5% participation rate) of their randomly selected community-dwelling, elderly patients who were taking 5 or more medications daily. In the intervention group, pharmacists conducted face-to-face medication reviews with the patients and then gave written recommendations to the physicians to resolve any drug-related problems. Process outcomes included the number of drug-related problems identified among the senior citizens in the intervention arm and the proportion of recommendations implemented by the physicians.
Results: After 5 months, seniors in the intervention and control groups were taking a mean of 12.4 and 12.2 medication units per day respectively (p = 0.50). There were no statistically significant differences in health care use or costs between groups. A mean of 2.5 drug-related problems per senior was identified in the intervention arm. Physicians implemented or attempted to implement 72.3% (790/1093) of the recommendations.
Interpretation: The intervention did not have a significant effect on patient outcomes. However, physicians were receptive to the recommendations to resolve drug-related problems, suggesting that collaboration between physicians and pharmacists is feasible.
Figures
Comment in
-
Why most interventions to improve physician prescribing do not seem to work.CMAJ. 2003 Jul 8;169(1):30-1. CMAJ. 2003. PMID: 12847036 Free PMC article. Review. No abstract available.
References
-
- Stewart RB. Polypharmacy in the elderly: a fait accompli? DICP: the annals of pharmacotherapy 1990;24:321-3. - PubMed
-
- Avorn J. Medication use and the elderly: current status and opportunities. Health Aff 1995;14:276-86. - PubMed
-
- Col N, Fanale JE, Konholm P. The role of medication noncompliance and adverse drug reactions in hospitalizations of the elderly. Arch Intern Med 1990; 150:841-5. - PubMed
-
- Bero LA, Lipton HL, Bird JA. Characterization of geriatric drug-related hospital readmissions. Med Care 1991;29:989-1003. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources