

Effects of fluticasone vs. fluticasone/salmeterol on airway calibre and airway hyperresponsiveness in mild persistent asthma
- PMID: 12848770
- PMCID: PMC1884325
- DOI: 10.1046/j.1365-2125.2003.01831.x
Effects of fluticasone vs. fluticasone/salmeterol on airway calibre and airway hyperresponsiveness in mild persistent asthma
Abstract
Aims: Inhaled corticosteroids alone or in combination with long acting beta2-agonists are indicated for use in mild persistent asthmatics. We set out to evaluate effects on airway hyperresponsiveness (AHR) and airway calibre using hydrofluoroalkane fluticasone/salmeterol (FP/SM) vs. double the dose of fluticasone alone (FP).
Methods: Fourteen mild persistent asthmatics completed a randomized double-blind crossover study with 1-week run-in and washout periods prior to treatments. Subjects received 3 weeks of FP 250 microg or FP 125 microg/SM 25 microg as 1 puff twice daily. Methacholine PD20 and lung function were measured after both baseline and treatment periods.
Results: There were no significant differences in baseline values prior to randomized treatments. Compared with pooled baseline, FP/SM and FP conferred improvements (P < 0.05) on methacholine PD20: 2.5 (95% confidence interval 1.7, 3.2) and 1.6 (0.8-2.3) doubling dose improvements, respectively; between FP/SM vs. FP there was a 0.9 (0.4, 1.4) doubling dose difference (P < 0.05). For forced expiratory volume in 1 s (FEV1), forced mid-expiratory flow (FEF25-75) and morning peak expiratory flow (PEF), FP/SM but not FP conferred improvements (P < 0.05) compared with pooled baseline, with FP/SM being greater than FP (P < 0.05): differences in FEV1 of 7.2% (3.8, 10.6) predicted, FEF25-75 of 11.2% (6.3, 16.1) predicted, and morning PEF of 17 L x min(-1)(1-32).
Conclusions: FP/SM conferred improvements on AHR and airway calibre, while twice the dose of FP improved only AHR in patients with mild asthma. The differential effects of FP/SM and FP suggest separate but complementary actions of the two moieties on airway inflammation and smooth muscle stabilization. This may explain the beneficial effects of combination inhalers on exacerbations.
Figures
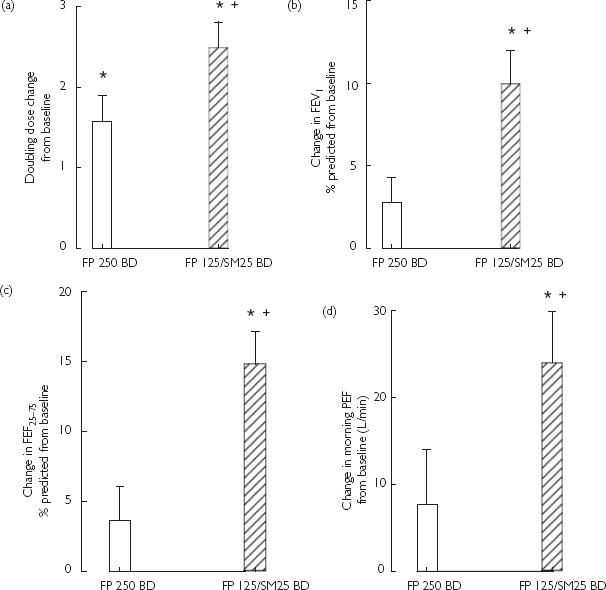
 ). *Significant (P < 0.05) difference from pooled baseline. †Significant (P < 0.05) difference between FP 125/SM 25 BD vs. FP 250 BD. (a) Methacholine doubling dose shift. (b) Forced expiratory volume in 1 s (FEV1) (% predicted). (c) FEF25−75 (% pre-dicted). (d) Morning PEF (L min−1).
). *Significant (P < 0.05) difference from pooled baseline. †Significant (P < 0.05) difference between FP 125/SM 25 BD vs. FP 250 BD. (a) Methacholine doubling dose shift. (b) Forced expiratory volume in 1 s (FEV1) (% predicted). (c) FEF25−75 (% pre-dicted). (d) Morning PEF (L min−1).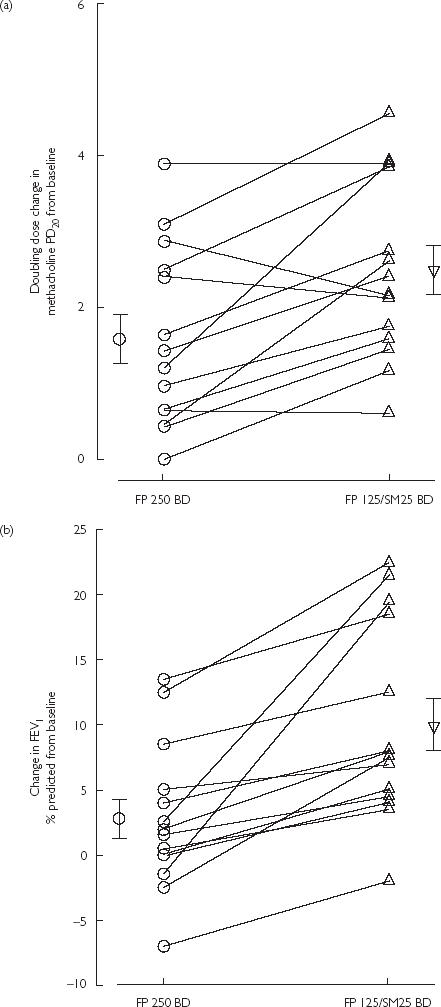
References
-
- O'Byrne PM, Barnes PJ, Rodriguez-Roisin R, et al. Low dose inhaled budesonide and formoterol in mild persistent asthma: the OPTIMA randomized trial. Am J Respir Crit Care Med. 2001;164:1392–1397. - PubMed
-
- Sont JK, Willems LN, Bel EH, et al. Clinical control and histopathologic outcome of asthma when using airway hyperresponsiveness as an additional guide to long-term treatment. The AMPUL Study Group. Am J Respir Crit Care Med. 1999;159:1043–1051. - PubMed
