

Prevalence of potential noninvasive arrhythmia risk predictors in healthy, middle-aged persons
- PMID: 12848812
- PMCID: PMC6932519
- DOI: 10.1046/j.1542-474x.2003.08107.x
Prevalence of potential noninvasive arrhythmia risk predictors in healthy, middle-aged persons
Abstract
Background: To date, prevalence and clinical significance of noninvasive arrhythmia risk predictors in apparently healthy, middle-aged persons are largely unknown.
Methods: A total of 110 apparently healthy persons 20-75 years old were enrolled in this prospective observational monocenter study and followed up for 32 +/- 15 months. Baseline investigations included symptom-limited bicycle ergometry, echocardiography, time-domain analysis, and spectral turbulence analysis of the signal-averaged electrocardiogram (ECG), ventricular arrhythmias, and heart rate variability on 24-hour Holter ECG, baroreflex sensitivity, and t-wave alternans in all persons.
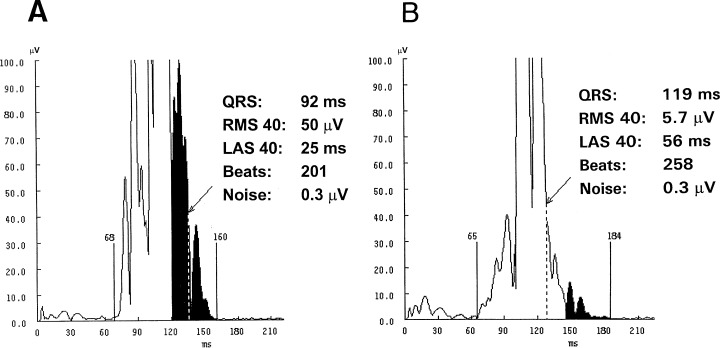
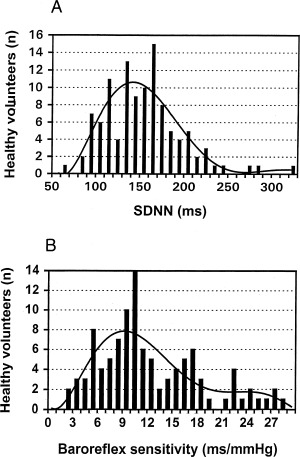
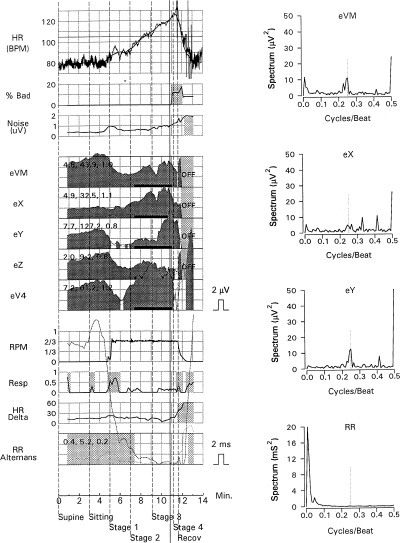
Results: The prevalence of an abnormal signal-averaged ECG was 1% for spectral turbulence analysis and varied between 1% and 37% for time-domain analysis depending upon the definition used for an abnormal time-domain analysis. A reduced heart rate variability defined as a standard deviation of normal-to-normal intervals < or =105 ms, <100 ms and <70 ms was found in 12%, 9%, and 1% of persons. A baroreflex sensitivity <6 ms/mmHg and <3 ms/mmHg was present in 15% and 2% of persons. Microvolt t-wave alternans was found to be positive in 5%, negative in 88%, and indeterminate in 7% of persons, respectively. During the 32 +/- 15 months follow-up, no arrhythmic events and no cardiovascular mortality were observed in this population.
Conclusions: Abnormal findings of noninvasive arrhythmia risk stratification can be found in 1-37% of healthy, middle-aged persons when previously reported cut-off values are used.
Figures
Similar articles
-
Noninvasive arrhythmia risk stratification in idiopathic dilated cardiomyopathy: design and first results of the Marburg Cardiomyopathy Study.Pacing Clin Electrophysiol. 1998 Nov;21(11 Pt 2):2551-6. doi: 10.1111/j.1540-8159.1998.tb01217.x. Pacing Clin Electrophysiol. 1998. PMID: 9825383
-
Noninvasive arrhythmia risk stratification in idiopathic dilated cardiomyopathy: results of the Marburg Cardiomyopathy Study.Circulation. 2003 Dec 9;108(23):2883-91. doi: 10.1161/01.CIR.0000100721.52503.85. Epub 2003 Nov 17. Circulation. 2003. PMID: 14623812
-
Relation between microvolt level T wave alternans and other potential noninvasive predictors of arrhythmic risk in the Marburg Cardiomyopathy Study.Pacing Clin Electrophysiol. 2000 Nov;23(11 Pt 2):1960-4. doi: 10.1111/j.1540-8159.2000.tb07062.x. Pacing Clin Electrophysiol. 2000. PMID: 11139967 Clinical Trial.
-
The clinical value of T-wave alternans derived from Holter monitoring.Europace. 2017 Apr 1;19(4):529-534. doi: 10.1093/europace/euw292. Europace. 2017. PMID: 28339589 Review.
-
Arrhythmic risk stratification of post-myocardial infarction patients.Curr Opin Cardiol. 2000 Jan;15(1):1-6. doi: 10.1097/00001573-200001000-00001. Curr Opin Cardiol. 2000. PMID: 10666655 Review.
Cited by
-
Electromuscular incapacitating devices discharge and risk of severe bradycardia.Am J Forensic Med Pathol. 2015 Jun;36(2):94-8. doi: 10.1097/PAF.0000000000000143. Am J Forensic Med Pathol. 2015. PMID: 25710795 Free PMC article.
-
Safety and tolerability of the novel inhaled corticosteroid fluticasone furoate in combination with the β2 agonist vilanterol administered once daily for 52 weeks in patients >=12 years old with asthma: a randomised trial.Thorax. 2013 Jun;68(6):513-20. doi: 10.1136/thoraxjnl-2012-202606. Epub 2013 Feb 25. Thorax. 2013. PMID: 23440247 Free PMC article. Clinical Trial.
-
T-wave alternans: reviewing the clinical performance, understanding limitations, characterizing methodologies.Ann Noninvasive Electrocardiol. 2008 Oct;13(4):401-20. doi: 10.1111/j.1542-474X.2008.00254.x. Ann Noninvasive Electrocardiol. 2008. PMID: 18973498 Free PMC article. Review.
-
Heart rate turbulence following ventricular premature beats in healthy controls.Ann Noninvasive Electrocardiol. 2003 Apr;8(2):127-31. doi: 10.1046/j.1542-474x.2003.08206.x. Ann Noninvasive Electrocardiol. 2003. PMID: 12848793 Free PMC article.
-
Influence of diabetes and/or myocardial infarction on prevalence of abnormal T-wave alternans.Ann Noninvasive Electrocardiol. 2009 Oct;14(4):355-9. doi: 10.1111/j.1542-474X.2009.00325.x. Ann Noninvasive Electrocardiol. 2009. PMID: 19804512 Free PMC article.
References
-
- Kuchar DL, Thorburn CW, Sammel NL. Prediction of serious arrhythmic events after myocardial infarction: Signal averaged electrocardiogram, Holter monitoring and radionuclide ventriculography. J Am Coll Cardiol 1987;9: 531–538. - PubMed
-
- Gomes JQ, Winters SL, Stewart D, et al. A new noninvasive index to predict sustained ventricular tachycardia and sudden death in the first year after myocardial infarction: Based on signal‐averaged electrocardiogram, radionuclide ejection fraction and Holter monitoring. J Am Coll Cardiol 1987;10: 349–357. - PubMed
-
- Gomes JA, Winters SL, Martinson M, et al. The prognostic significance of quantitative signal‐averaged variables relative to clinical variables, site of myocardial infarction, ejection fraction and ventricular premature beats: A prospective study. J Am Coll Cardiol 1989;13: 377–384. - PubMed
-
- Breithardt G, Cain ME, El‐Sherif N, et al. Standards for analysis of ventricular late potentials using high‐resolution or signal‐averaged electrocardiography. A statement of the European Society of Cardiology, the American Heart Association, and the American College of Cardiology. J Am Coll Cardiol 1991;17: 999–1006. - PubMed
-
- Bigger JT Jr, for the Coronary Artery Bypass Graft Patch Trial Investigators . Prophylactic use of implanted cardiac defibrillators in patients at high risk for ventricular arrhythmias after coronary artery bypass graft surgery. N Engl J Med 1997;337: 1569–1575. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
