

Depressive symptoms and health-related quality of life: the Heart and Soul Study
- PMID: 12851276
- PMCID: PMC2776689
- DOI: 10.1001/jama.290.2.215
Depressive symptoms and health-related quality of life: the Heart and Soul Study
Abstract
Context: Little is known regarding the extent to which patient-reported health status, including symptom burden, physical limitation, and quality of life, is determined by psychosocial vs physiological factors among patients with chronic disease.
Objective: To compare the contributions of depressive symptoms and measures of cardiac function to the health status of patients with coronary artery disease.
Design, setting, and participants: Cross-sectional study of 1024 adults with stable coronary artery disease recruited from outpatient clinics in the San Francisco Bay Area between September 2000 and December 2002. Main Measures Measurement of depressive symptoms using the Patient Health Questionnaire (PHQ); assessment of cardiac function by measuring left ventricular ejection fraction on echocardiography, exercise capacity on treadmill testing, and ischemia on stress echocardiography; and measurement of a range of health status outcomes, including symptom burden, physical limitation, and quality of life, using the Seattle Angina Questionnaire. Participants were also asked to rate their overall health as excellent, very good, good, fair, or poor.
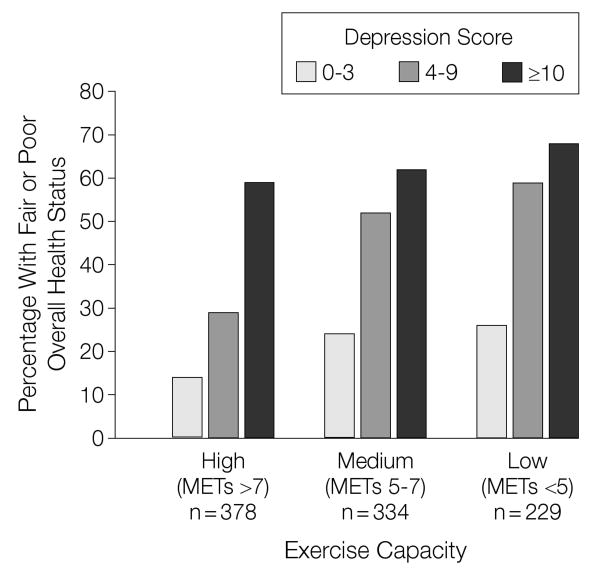
Results: Of the 1024 participants, 201 (20%) had depressive symptoms (PHQ score > or =10). Participants with depressive symptoms were more likely than those without depressive symptoms to report at least mild symptom burden (60% vs 33%; P<.001), mild physical limitation (73% vs 40%; P<.001), mildly diminished quality of life (67% vs 31%; P<.001), and fair or poor overall health (66% vs 30%; P<.001). In multivariate analyses adjusting for measures of cardiac function and other patient characteristics, depressive symptoms were strongly associated with greater symptom burden (odds ratio [OR], 1.8; 95% confidence interval [CI], 1.3-2.7; P =.002), greater physical limitation (OR, 3.1; 95% CI, 2.1-4.6; P<.001), worse quality of life (OR, 3.1; 95% CI, 2.2-4.6; P<.001), and worse overall health (OR, 2.0; 95% CI, 1.3-2.9; P<.001). Although decreased exercise capacity was associated with worse health status, left ventricular ejection fraction and ischemia were not.
Conclusions: Among patients with coronary disease, depressive symptoms are strongly associated with patient-reported health status, including symptom burden, physical limitation, quality of life, and overall health. Conversely, 2 traditional measures of cardiac function-ejection fraction and ischemia-are not. Efforts to improve health status should include assessment and treatment of depressive symptoms.
Figures

Comment in
-
Depression and health-related quality of life.JAMA. 2003 Nov 12;290(18):2404; author reply 2404. doi: 10.1001/jama.290.18.2404-a. JAMA. 2003. PMID: 14612467 No abstract available.
References
-
- Coronary Artery Surgery Study (CASS): a randomized trial of coronary artery bypass surgery: quality of life in patients randomly assigned to treatment groups. Circulation. 1983;68:951–960. - PubMed
-
- Croog SH, Levine S, Testa MA, et al. The effects of antihypertensive therapy on the quality of life. N Engl J Med. 1986;314:1657–1664. - PubMed
-
- Hlatky MA, Rogers WJ, Johnstone I, et al. Medical care costs and quality of life after randomization to coronary angioplasty or coronary bypass surgery: Bypass Angioplasty Revascularization Investigation (BARI) Investigators. N Engl J Med. 1997;336:92–99. - PubMed
-
- Pilote L, Lauzon C, Huynh T, et al. Quality of life after acute myocardial infarction among patients treated at sites with and without on-site availability of angiography. Arch Intern Med. 2002;162:553–559. - PubMed
-
- Sjoland H, Wiklund I, Caidahl K, Albertsson P, Herlitz J. Relationship between quality of life and exercise test findings after coronary artery bypass surgery. Int J Cardiol. 1995;51:221–232. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
