

Laparoscopic total mesorectal excision of low rectal cancer with preservation of anal sphincter: a report of 82 cases
- PMID: 12854145
- PMCID: PMC4615486
- DOI: 10.3748/wjg.v9.i7.1477
Laparoscopic total mesorectal excision of low rectal cancer with preservation of anal sphincter: a report of 82 cases
Abstract
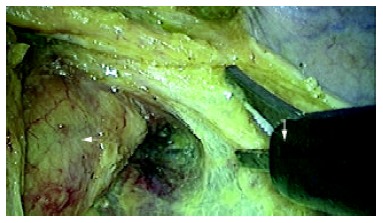
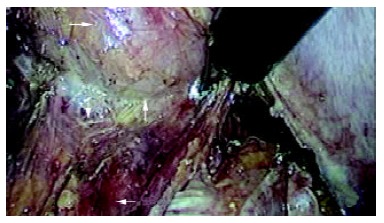
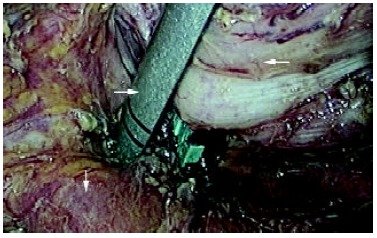
Aim: To assess the feasibility and efficacy of laparoscopic total mesorectal excision (LTME) of low rectal cancer with preservation of anal sphincter.
Methods: From June 2001 to June 2003, 82 patients with low rectal cancer underwent laparoscopic total mesorectal excision with preservation of anal sphincter. The lowest edge of tumors was below peritoneal reflection and 1.5-7 cm from the dentate line (1.5-5 cm in 48 cases, 5-7 cm in 34 cases).
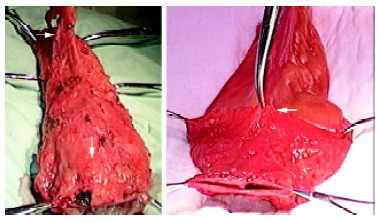
Results: LTME with anal sphincter preservation was performed on 82 randomized patients with low rectal cancer, and 100 % sphincter preservation rate was achieved. There were 30 patients with laparoscopic low anterior resection (LLAR) at the level of the anastomosis below peritoneal reflection and 2 cm above from the dentate line; 27 patients with laparoscopic ultralow anterior resection (LULAR) at the level of anastomoses 2 cm below from the dentate line; and 25 patients with laparoscopic coloanal anastomoses (LCAA) at the level of the anastomoses at or below the dentate line. No defunctioning ileostomy was created in any case. The mean operating time was 120 minutes (ranged from 110-220 min), and the mean operative blood loss was 20 mL (ranged from 5-120 mL). Bowel function was restored and diet was resumed on day 1 or 2 after operation. The mean hospital stay was 8 days (ranged from 5-14). Postoperative analgesics were used in 45 patients. After surgery, 2 patients had urinary retention, one had anastomotic leakage, and another 2 patients had local recurrence one year later. No interoperative complication was observed.
Conclusion: LTME with preservation of anal sphincter is a feasible, safe and minimally invasive technique with less postoperative pain and rapid recovery, and importantly, it has preserved the function of the sphincter.
Figures


References
-
- Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery--the clue to pelvic recurrence. Br J Surg. 1982;69:613–616. - PubMed
-
- Goldberg S, Klas JV. Total mesorectal excision in the treatment of rectal cancer: a view from the USA. Semin Surg Oncol. 1998;15:87–90. - PubMed
-
- MacFarlane JK, Ryall RD, Heald RJ. Mesorectal excision for rectal cancer. Lancet. 1993;341:457–460. - PubMed
-
- Ceelen W, Pattyn P. Total mesorectal excision in the treatment of rectal cancer: a review. Acta Chir Belg. 2000;100:94–99. - PubMed
-
- Kapiteijn E, van De Velde CJ. European trials with total mesorectal excision. Semin Surg Oncol. 2000;19:350–357. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
