

Assessment of whether in-hospital mortality for lobectomy is a useful standard for the quality of lung cancer surgery: retrospective study
- PMID: 12855523
- PMCID: PMC164918
- DOI: 10.1136/bmj.327.7406.73
Assessment of whether in-hospital mortality for lobectomy is a useful standard for the quality of lung cancer surgery: retrospective study
Abstract
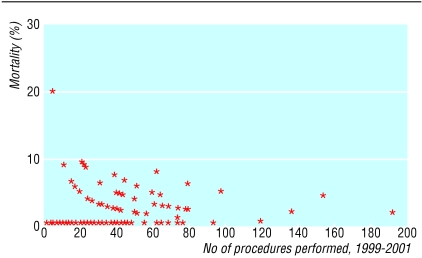
Objectives: To calculate in-hospital mortality after lobectomy for primary lung cancer in the United Kingdom; to explore the validity of using such data to assess the quality of UK thoracic surgeons; and to investigate the relation between in-hospital mortality and the number of procedures performed by surgeons.
Design: Retrospective study.
Setting: 36 departments dealing with thoracic surgery in UK hospitals.
Participants: 4028 patients who had undergone lobectomy for primary lung cancer by one of 102 surgeons.
Main outcome measures: In-hospital mortality in relation to individual surgeons, among all patients, and among each of five groups of patients defined by the number of operations performed by the surgeon.
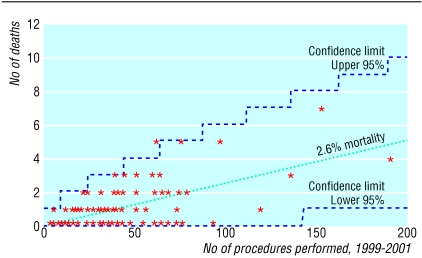
Results: 103 patients (2.6%, 95% confidence interval 2.1% to 3.1%) died after surgery during the same hospital admission. No significant difference was found for in-hospital mortality between the five groups.
Conclusions: The number of procedures performed by a thoracic surgeon is not related to in-hospital mortality. Reporting data on in-hospital mortality after lobectomy for primary lung cancer is a poor tool for measuring a surgeon's performance.
Figures
References
-
- Birkmeyer JD, Siewers AE, Finlayson EV, Stukel TA, Lucas FL, Batista I, et al. Hospital volume and surgical mortality in the United States. N Engl J Med 2002;346: 1128-37. - PubMed
-
- Bach PB, Cramer LD, Schrag D, Downey RJ, Gelfand SE, Begg CB. The influence of hospital volume on survival after resection for lung cancer. N Engl J Med 2001;345: 181-8. - PubMed
-
- Gawande A. The learning curve. New Yorker Jan 28, 2002: 52-61.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical