

Virtual outreach: economic evaluation of joint teleconsultations for patients referred by their general practitioner for a specialist opinion
- PMID: 12855528
- PMCID: PMC164917
- DOI: 10.1136/bmj.327.7406.84
Virtual outreach: economic evaluation of joint teleconsultations for patients referred by their general practitioner for a specialist opinion
Abstract
Objectives: To test the hypotheses that, compared with conventional outpatient consultations, joint teleconsultation (virtual outreach) would incur no increased costs to the NHS, reduce costs to patients, and reduce absences from work by patients and their carers.
Design: Cost consequences study alongside randomised controlled trial.
Setting: Two hospitals in London and Shrewsbury and 29 general practices in inner London and Wales.
Participants: 3170 patients identified; 2094 eligible for inclusion and willing to participate. 1051 randomised to virtual outreach and 1043 to standard outpatient appointments.
Main outcome measures: NHS costs, patient costs, health status (SF-12), time spent attending index consultation, patient satisfaction.
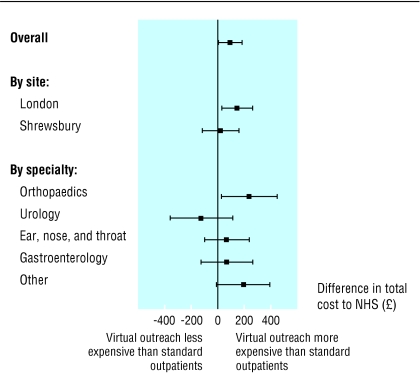
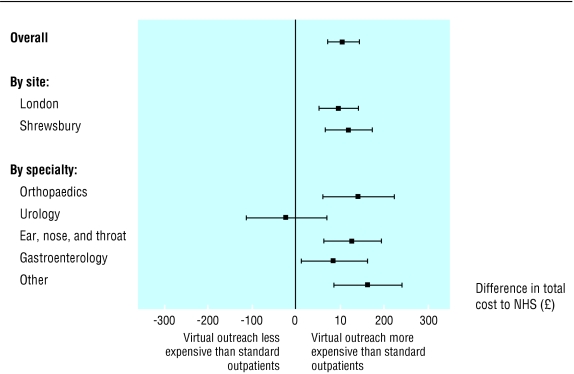
Results: Overall six months costs were greater for the virtual outreach consultations ( pound 724 per patient) than for conventional outpatient appointments ( pound 625): difference in means pound 99 ($162; 138) (95% confidence interval pound 10 to pound 187, P=0.03). If the analysis is restricted to resource items deemed "attributable" to the index consultation, six month costs were still greater for virtual outreach: difference in means pound 108 ( pound 73 to pound 142, P < 0.0001). In both analyses the index consultation accounted for the excess cost. Savings to patients in terms of costs and time occurred in both centres: difference in mean total patient cost pound 8 ( pound 5 to pound 10, P < 0.0001). Loss of productive time was less in the virtual outreach group: difference in mean cost pound 11 ( pound 10 to pound 12, P < 0.0001).
Conclusion: The main hypothesis that virtual outreach would be cost neutral is rejected, but the hypotheses that costs to patients and losses in productivity would be lower are supported.
Figures
References
-
- Roland M. Measuring referral rates. In: Roland M, Coulter A, eds. Hospital referrals. Oxford: Oxford University Press, 1992: 62-75.
-
- Wallace P, Hopkins A, eds. Referral to medical outpatients—different agendas of patients, general practitioners and hospital physicians. London: Royal College of Physicians, 1992.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources