

Borna disease virus infection, a human mental-health risk
- PMID: 12857781
- PMCID: PMC164222
- DOI: 10.1128/CMR.16.3.534-545.2003
Borna disease virus infection, a human mental-health risk
Abstract
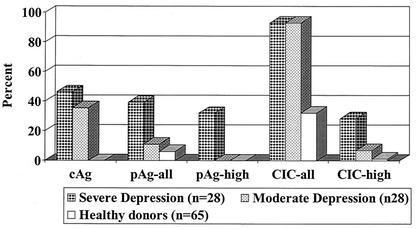
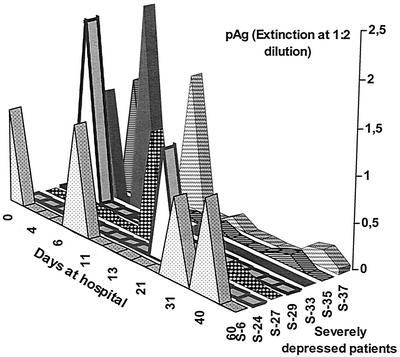
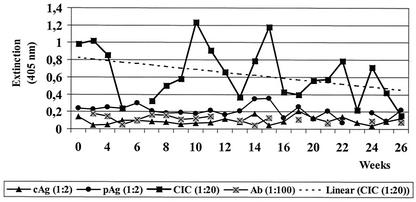
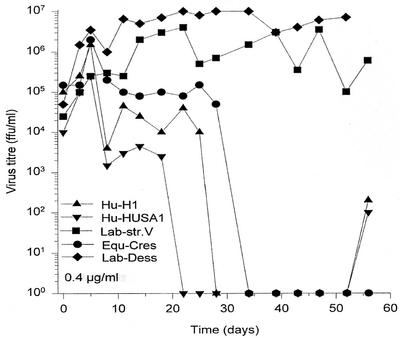
This article focuses on human Borna disease virus (BDV) infections, most notably on the development of valid diagnostic systems, which have arisen as a major research issue in the past decade. The significance of a novel modular triple enzyme-linked immunosorbent assay that is capable of specifically measuring anti-BDV antibodies as well as major structural proteins N (p40) and P (p24) in the blood, either as free antigens in the plasma or as antibody-bound circulating immune complexes (CICs), is explained. The impact of CICs and plasma antigen, which indicate periods of antigenemia in the course of BDV infection, along with other infection markers that are still in use is discussed. The review further provides new insight into possible links of BDV to human diseases, summarizing cross-sectional and longitudinal data which correlate acute depression with the presence and amount of antigen and CICs. Moreover, BDV prevalence in healthy people is reevaluated, suggesting that this was previously underestimated. Antiviral efficacy of amantadine, in vivo and in vitro, is outlined as well, with emphasis on wild-type (human and equine) versus laboratory strains. Finally, the pros and cons of the association of BDV with human disease, as detailed in the literature, are critically discussed and related to our data and concepts. This article supports existing correlative evidence for a pathogenic role of BDV infection in particular human mental disorders, in analogy to what has been proven for a variety of animal species.
Figures

References
-
- Allmang, U., M. Hofer, S. Herzog, K. Bechter, and P. Staeheli. 2001. Low avidity of human serum antibodies for Borna disease virus antigens questions their diagnostic value. Mol. Psychiatry 6:329-333. - PubMed
-
- Bechter, K. 1998. Borna Disease Virus, mögliche Ursache neurologischer Störungen des Menschen. Monographien aus dem Gesamtgebiet der Psychiatrie. Steinkopff, Darmstadt, Germany.
-
- Billich, C., et al. 2002. Biol. Psychiatry 51:979-987. - PubMed
-
- Bode, L., F. Steinbach, and H. Ludwig. 1994. A novel marker for Borna disease virus infection. Lancet 343:297-298. - PubMed
-
- Bode, L., W. Zimmermann, R. Ferszt, F. Steinbach, and H. Ludwig. 1995. Borna disease virus genome transcribed and expressed in psychiatric patients. Nat. Med. 1:232-236. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
