

Review
doi: 10.1136/heart.89.8.949.
Development of the heart: (2) Septation of the atriums and ventricles
Affiliations
- PMID: 12860885
- PMCID: PMC1767797
- DOI: 10.1136/heart.89.8.949
Item in Clipboard
Review
Development of the heart: (2) Septation of the atriums and ventricles
Heart.
2003 Aug.
No abstract available
Figures

This adult human heart has been sectioned in “four chamber” plane to reveal the nature of the rims of the oval fossa (fossa ovalis). The floor of the fossa is the flap valve, which if removed would create a communication between right and left atriums. The infero-anterior rim (red dotted lines) is a muscular buttress that can also be removed to create a communication between the chambers. The extensive superior rim (yellow dotted lines), however, is a fold between the attachments of the caval veins to the right atrium and the pulmonary veins to the left atrium. Cutting through this rim would create a communication with the extracardiac space.

The upper panel (A) is another “four-chamber” section through an adult human heart, this time taken closer to the crux. It shows the area of off-setting between the hinges of the tricuspid (blue and yellow arrow) and mitral (red and yellow arrow) valves. Initially, we described this area as a muscular “septum”. As can be seen in the section, however, extracardiac adipose tissue is incorporated between the layers of atrial and ventricular musculature, producing a notably different anatomic arrangement separating the atrial cavities when compared to the flap valve (double headed arrow) or the muscular buttress (star) at the base of the flap valve. The lower panel (B) shows a view of the short axis of the cardiac mass along the plane B–B in fig 2A, viewed from the atrial aspect. It shows the origin and extent of the extracardiac adipose tissue, which extends anteriorly and superiorly between the atrial and ventricular muscle masses from the inferior atrioventricular groove (star), with the artery to the atrioventricular node coursing through the tissue plane thus created. The yellow dotted lines show the cut edges of the atrial musculature, and the bracket shows the site of the membranous septum, which has been removed.

These sections in transverse plane across the embryo are from a human embryo measuring 4 mm from crown to rump, at the 12th stage according to the Carnegie classification. Panel A shows the right and left sinus horns at their attachment to the primary atrium, with the dorsal, or posterior, mesocardium connecting the primary atrium itself to the posterior wall of the embryo. At this stage, there is only minimal formation of the lung buds, with the right bud just visible in panel B. This panel, taken slightly more inferiorly compared to panel A, shows the fold between the two sinus horns (RSH, LSH) at their junction with the primary atrium. This is the so-called “septum” of the embryonic systemic venous sinus.

These panels show the fate of the so-called “septum” of the systemic venous sinus. Panel A is from a mouse embryo on the 10th day of development. The star shows the tissue separating the mouths of the right and left sinus horns at their junction with the primary atrium. Note the dorsal mesocardium, and compare with panel B of fig 3. Panel B is from a human embryo at stage 20 of the Carnegie classification, sectioned more or less in parasternal long axis plane. It shows the fold between the entrance of the coronary sinus (CS), derived from the left sinus horn, and that of the inferior caval vein (ICV), formed from the lower end of the opening of the right sinus horn. This fold is the so-called “septum” of the systemic venous sinus.

This picture shows the atrioventricular canal in a mouse heart during the 10th day of development, viewed from above having transected the developing heart tube. Note the cushions filling the common atrioventricular canal, and growing towards each other from the superior and inferior quadrants. Note also that the outflow tract is a solitary tube at this stage, also with opposing cushions developing within its lumen.

This section, in parasternal long axis plane, is from a human embryo at stage 14 of the Carnegie classification. The endocardial cushions (SC, IC) have formed superiorly and inferiorly within the atrioventricular canal, which at this stage has appreciable length. The left sinus horn (LSH) is now incorporated as a channel with its own walls within the developing left atrioventricular junction. The primary septum itself has grown down from the atrial roof, but has broken down superiorly to produce the secondary interatrial foramen (2F). The primary foramen is seen between the primary septum and the as yet unfused atrioventricular cushions. The section shows also the window for growth into the heart from the posterior mediastinum (yellow and red arrow). This is the vestibular spine.

This section, in “four chamber” plane, is from a human embryo at stage 16 of the Carnegie classification. The section has passed through the superior cushion of the atrioventricular (AV) canal, which has yet to fuse with its partner. The primary atrial septum has grown down from the atrial roof, carrying a mesenchymal cap on its leading edge. Note, however, that the upper edge of the primary septum has already broken down to form the secondary interatrial foramen. The primary foramen is still patent, between the mesenchymal cap and the atrial surface of the atrioventricular cushions.

This scanning electron micrograph is from a mouse heart at a slightly earlier stage of development than the human embryo shown in fig 6. The atrioventricular canal has been dissected away from the atrial chambers, permitting the atrial cavities to be photographed from beneath. The valves of the systemic venous sinus have now formed, showing that the sinus itself (SVS) opens exclusively to the right side of the primary atrium. Note that the orifice of the pulmonary vein now opens inferiorly to the left side of the atrium. The primary atrial septum is growing as a shelf between the systemic and pulmonary venous orifices. Note also the bulge at the right side of the pulmonary venous orifice, between it and the opening of the systemic venous sinus. This is the “spina vestibuli” initially described by His,9 which we term the vestibular spine.

This higher power scanning electron micrograph shows the atrial roof, prepared in comparable fashion to fig 8, but at a slightly later stage of development. The upper margin of the primary atrial foramen has now broken down to form the secondary interatrial foramen (double headed arrow). Note the mesenchymal cap on the leading edge of the primary septum, which is growing towards the atrioventricular endocardial cushions, carrying forward the inferior end of the orifice of the systemic venous sinus (star). The upper end of the orifice becomes the septum spurium in the roof of the right atrial appendage.

This section, in four chamber plane, is from a human embryo at stage 16 of the Carnegie classification. It shows how the mesenchymal cap on the primary atrial septum has now fused with the superior cushion, with breakdown of the upper edge to form the secondary foramen. The upper margin of the foramen, however, is flat to the orifice of the right sinus horn (RSH, black line). Only subsequent to septation is there infolding of the superior margin (see fig 12).

This section, in four chamber plane, is from the same human embryo at stage 16 of the Carnegie classification as shown in fig 10. This section shows the inferior cushion adherent to the ventricular septum, but with the larger part of its bulk within the left ventricle. It also shows the tissue growing into the heart through the vestibular spine, confining the pulmonary vein within the developing left atrium. Note the left sinus horn (LSH) with its own discrete walls.

This section is from a human embryo in the eighth week of development, subsequent to the completion of septation. Only at this stage are the right and left pulmonary veins (RPV, LPV) separating and becoming incorporated in the posterior wall of the left atrium. Also only at this stage is there folding of the superior atrial wall (yellow and red arrow) to produce the so-called “septum secundum”, in reality part of the interatrial fold. By this stage, the mesenchymal mass formed by fusion of the vestibular spine and mesenchymal cap on the primary atrial septum has muscularised, leaving the central core as the fibrous tendon of Todaro. Note the separate walls of the left sinus horn (LSH).

This short axis section is taken from a human heart in the eighth week of development, subsequent to the completion of septation. It shows how the fused atrioventricular cushions have now formed the atrioventricular component of the membranous septum interposed between right atrium and subaortic vestibule (double headed arrow), and also the aortic leaflet of the mitral valve (red and yellow star). Inf., subpulmonary infundibulum; LA, left atrium.

This section, in oblique short axis plane, is from a human embryo at Carnegie stage 22, just subsequent to the completion of septation. It is taken through the newly developed atrioventricular septal area, and has cut through the initial atrioventricular canal musculature that persists as the atrioventricular conduction axis (yellow dotted lines). The superior part of the musculature is now the atrioventricular bundle, with the inferior part becoming sequestrated within the atrial myocardium as the atrial wall folds over the ventricular muscle mass (yellow and red arrow). The fused central parts of the endocardial cushions have now become the central fibrous body.

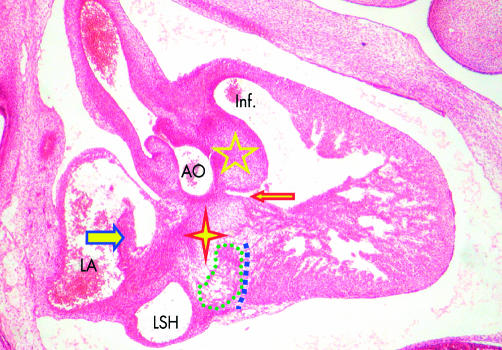
This section, in parasternal long axis plane, is from a human embryo at Carnegie stage 20. Ventricular septation is almost complete, and in this plane, the lower end of the outflow cushions (star), separating the subaortic vestibule (AO) from the subpulmonary infundibulum (Inf.), has fused with the muscular ventricular septum (red dashed line), the septum carrying on its crest the axis of atrioventricular conduction tissue (yellow dotted lines). In the area of the septal atrioventricular junction, the endocardial cushions have fused to form the central fibrous body (red asterisk), but note that the musculature of the inner heart curve still separates the developing leaflets of the aortic valve from the fibrous tissue (green dashed line). The area of formation of the atrioventricular muscular sandwich is seen inferior to the fibrous body, where the initial musculature of the atrioventricular canal (large orange asterisk) is disappearing in the region of formation of the inferior atrioventricular groove (blue dashed line). Note how the left sinus horn (LSH) is now incorporated within the left atrioventricular groove.

This section, from a human embryo in the eighth week of development, subsequent to the completion of septation, is again sectioned in parasternal long axis plane. It shows that the antero-superior leaflet of the tricuspid valve (red and yellow arrow) has now formed within the cavity of the right ventricle. The central fibrous body, formed by fusion of the atrioventricular cushions, now forms the atrioventricular component of the membranous septum (red and yellow double headed arrow). The interventricular part of the membranous septum (blue and yellow arrow) is developing from the proximal end of the fused outflow cushions, the remainder of the cushions having muscularised at this stage to form the supraventricular crest (SVC). A tissue plane will form along the line of red dots eventually to separate part of the crest from the aorta (AO) as the free standing subpulmonary infundibulum.
This section, in parasternal long axis plane, is from a human embryo at Carnegie stage 20, just before final closure of the interventricular foramen (red and yellow arrow). The proximal end of the fused outflow cushions (five pointed star) is dividing the subpulmonary infundibulum (Inf.) from the subaortic vestibule. The outflow cushions have almost fused with the central fibrous body formed by fusion of the atrioventricular endocardial cushions (four pointed star). Beneath the central fibrous body, the atrioventricular canal musculature (green dotted line) is being sequestrated as the vestibule of the right atrium by formation of the inferior atrioventricular groove (blue dotted line). The primary atrial septum (blue and yellow arrow) is attached to the atrial aspect of the fibrous body, with the left sinus horn (LSH) forming the coronary sinus in the left atrioventricular groove. Note the maturation of the superior end of the atrioventricular canal musculature to form the atrioventricular node.

This scanning electron micrograph, from a mouse embryo with 42 somites, shows the formation of the muscular ventricular septum. The specimen was prepared by transecting the heart through the atrioventricular canal, and the photograph is of the posterior segment. Note the inferior cushion (IC) occupying most of the posterior margin of the canal, but note also that the floor of the right atrium is in continuity with the roof of the developing right ventricle at the right margin of the atrioventricular canal, even though the atrioventricular groove interposes between the cavities of right atrium and right ventricle (yellow dashed line). Ballooning of the apical parts of the right and left ventricles from the ascending and descending parts of the ventricular component of the primary heart tube, respectively, has produced the primary muscular ventricular septum between them (star). The primary ventricular foramen (yellow bracket) provides the entrance at this stage to the developing right ventricle.

This section from a human embryo at Carnegie stage 14 is comparable to the picture of the mouse heart shown in fig 18. This section, however, has been stained with an antibody to the nodose ganglion of the chick, which recognises the developing atrioventricular conduction tissues, staining them brown. As can be seen, the conduction tissues at this stage form a ring around the primary interventricular foramen (double headed arrow), the inferior part of the ring marking the crest of the developing muscular ventricular septum, and the superior part occupying the right atrioventricular junction. Thus, at this stage the ring is both interventricular and atrioventricular. The section is taken between the unfused atrioventricular cushions, showing that most of the circumference of the atrioventricular canal is supported by the developing left ventricle (black bracket).

This section, in comparable plane to fig 19, is from a human embryo at stage 20, again stained with the antibody to the nodose ganglion of the chick. The atrial septum (red asterisk) has now fused with the central fibrous body, dividing right and left atriums (RA, LA). Expansion of the right atrioventricular junction has proceeded concomitant with formation of the inlet of the right ventricle (RV). The ring of atrioventricular conduction tissue is still placed on the crest of the ventricular septum (red and yellow arrow), but the expanded right part of the ring (blue and yellow arrow) is now becoming sequestrated in the vestibule of the right atrium by formation of the parietal right atrioventricular junction (red dotted line). This shows that the entirety of the right ventricle is formed from the tissues initially distal to the embryonic interventricular foramen. The section also shows that the superior part of the ring has been transferred to the left ventricle (LV) as the subaortic vestibule (AO, purple arrows). This will be committed to the left ventricle by eventual fusion of the atrioventricular and outflow cushions along the plane of the double headed purple and yellow arrow, converting the initial embryonic interventricular foramen into the subaortic vestibule.
References
-
- Moorman AFM, Webb S, Brown NA, et al. The development of the heart: (1) Formation of the cardiac chambers and arterial trunks. Heart 2003;89:806–14. ▸ In this, the first of our reviews, we discussed the steps involved in formation of the heart tube and the components of the cardiac chambers and arterial trunks. - PMC - PubMed
-
- Larsen WJ. Human embryology. New York: Churchill Livingstone 1993;147. ▸ This otherwise excellent student textbook of embryology used the “classical” account for development of the atrial septum, with purported primary and secondary septums illustrated as overlapping sheets that have grown into the heart.
-
- Anderson RH, Brown NA. The anatomy of the heart revisited. Anat Rec 1996;62:710–16. ▸ The review in which we questioned the definition of septal structures, arguing that it should be possible to resect a “true” septum without exiting from the cavities of the heart.
-
- Becker AE, Anderson RH. Atrioventricular septal defects. What’s in a name? J Thorac Cardiovasc Surg 1982;83:461–9. ▸ This review has proved seminal in the classification of hearts with common atrioventricular junction. In retrospect, however, we were wrong when we argued that, in addition to the fibrous atrioventricular septum, there was also a muscular septum. We now know that the purported muscular septum is, in reality, a layer of extracardiac fibroadipose tissue sandwiched between the atrial and ventricular walls. - PubMed
-
- Webb S, Kanani M, Anderson RH, et al. Development of the human pulmonary vein and its incorporation in the morphologically left atrium. Cardiol Young 2001;11:632–42. ▸ In this study, we showed how the pulmonary vein canalised as a new structure in the medistinal tissues, using the dorsal mesocardium to gain entrance to the primary atrial compartment of the heart tube. Only much later are the walls of the separate veins incorporated to form the dome of the left atrium. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources