

Platelet count/spleen diameter ratio: proposal and validation of a non-invasive parameter to predict the presence of oesophageal varices in patients with liver cirrhosis
- PMID: 12865282
- PMCID: PMC1773759
- DOI: 10.1136/gut.52.8.1200
Platelet count/spleen diameter ratio: proposal and validation of a non-invasive parameter to predict the presence of oesophageal varices in patients with liver cirrhosis
Abstract
Background and aims: Cirrhotic patients frequently undergo screening endoscopy for the presence of oesophageal varices (OV). In the future, this social and medical burden will increase due to the greater number of patients with chronic liver disease and their improved survival. In this study, our aims were (1) to identify clinical, biochemical, and ultrasonographic parameters which might non-invasively predict the presence of OV in patients with liver cirrhosis; (2) to evaluate the reproducibility of the obtained results in a different, although related, further group of patients; and (3) to assess the predictiveness of the identified rules in patients with compensated cirrhosis.
Methods: In the first part of the study we retrospectively evaluated the presence of OV in 145 cirrhotic patients, and in the second part we evaluated the reproducibility of the study results in a subsequent group of 121 patients. Finally, we evaluated these parameters in a subgroup of 145 patients with compensated disease. All 266 patients underwent a complete biochemical workup, upper digestive endoscopy, and ultrasonographic measurement of spleen bipolar diameter. Platelet count/spleen diameter ratio was calculated for all patients.
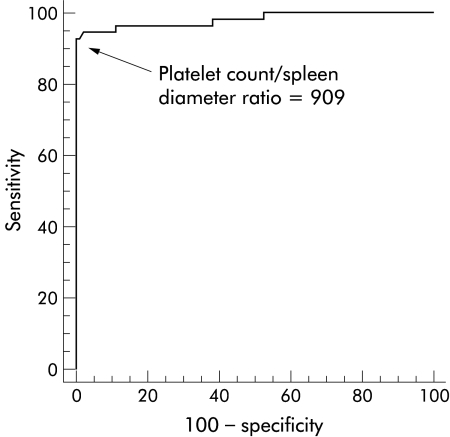
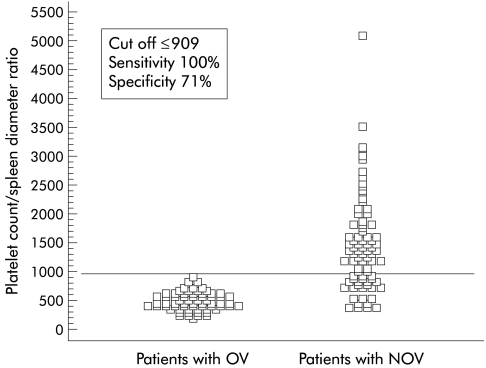
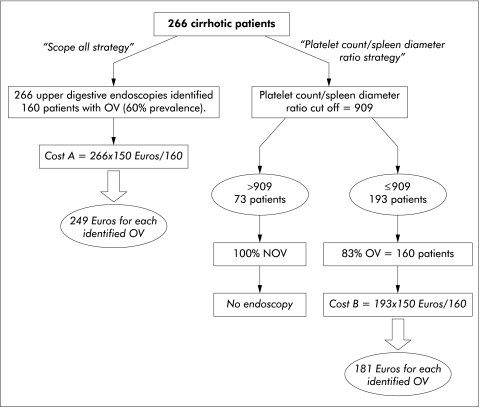
Results: The prevalence rates of OV were 61% and 58% in the first and second groups of patients, respectively. In the first part of the study, we found that platelet count, spleen diameter, platelet count/spleen diameter ratio, and Child- Pugh class were significantly different among patients with or without OV, although the platelet count/spleen diameter ratio was the only parameter which was independently associated with the presence of OV in a multivariate analysis. A platelet count/spleen diameter ratio cut off value of 909 had 100% negative predictive value for a diagnosis of OV. This result was reproduced in the second group of patients as well as in patients with compensated disease. In a cost-benefit analysis, screening cirrhotic patients according to the "platelet count/spleen diameter ratio strategy" was far more cost effective compared with the "scope all strategy".
Conclusions: The platelet count/spleen diameter ratio is the only parameter which is independently associated with the presence of OV, and its negative predictive value is reproducible. Its use is of value even in the subgroup of patients with compensated disease, and it is also cost effective.
Figures
Comment in
-
Platelet count/spleen diameter ratio predicted the presence of esophageal varices in liver cirrhosis.ACP J Club. 2004 Mar-Apr;140(2):53. ACP J Club. 2004. PMID: 15122873 No abstract available.
-
Prediction of oesophageal varices with platelet count/spleen diameter ratio or platelets alone.Gut. 2004 Jun;53(6):913-4; author reply 914-5. Gut. 2004. PMID: 15138224 Free PMC article. No abstract available.
-
Platelet count/spleen diameter ratio as a predictor of oesophageal varices in alcoholic cirrhosis.Gut. 2004 Jul;53(7):1055. Gut. 2004. PMID: 15194662 Free PMC article. No abstract available.
-
Infallibility of a normal platelet count/spleen diameter ratio in ruling out oesophageal varices?Gut. 2004 Nov;53(11):1721. Gut. 2004. PMID: 15479701 Free PMC article. No abstract available.
-
Right liver lobe diameter:albumin ratio: a new non-invasive parameter for prediction of oesophageal varices in patients with liver cirrhosis (preliminary report).Gut. 2007 Aug;56(8):1166-7; authro reply 1167. Gut. 2007. PMID: 17625152 Free PMC article. No abstract available.
References
-
- De Franchis R, Primignani M. Natural history of portal hypertension in patients with cirrhosis. Clin Liver Dis 2001;5:645–63. - PubMed
-
- Garceau AJ, Chalmers TC. The Boston Inter-Hospital Liver Group. The natural history of cirrhosis: I. Survival with oesophageal varices. N Engl J Med 1963;268:469–73. - PubMed
-
- Graham D, Smith JL. The course of patients after variceal hemorrhage. Gastroenterology 1981;80;800–9. - PubMed
-
- Rigo GP, Merighi A, Chalen JN, et al. A prospective study of the ability of three endoscopic classifications to predict hemorrhage from esophageal varices. Gastrointest Endosc 1992;38:425–9. - PubMed
-
- Jensen DM. Endoscopic screening for varices in cirrhosis: findings, implications, and outcomes. Gastroenterology 2002;122:1620–30. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical