

Prognostic factors for patients with hepatic metastases from breast cancer
- PMID: 12865918
- PMCID: PMC2394248
- DOI: 10.1038/sj.bjc.6601038
Prognostic factors for patients with hepatic metastases from breast cancer
Abstract
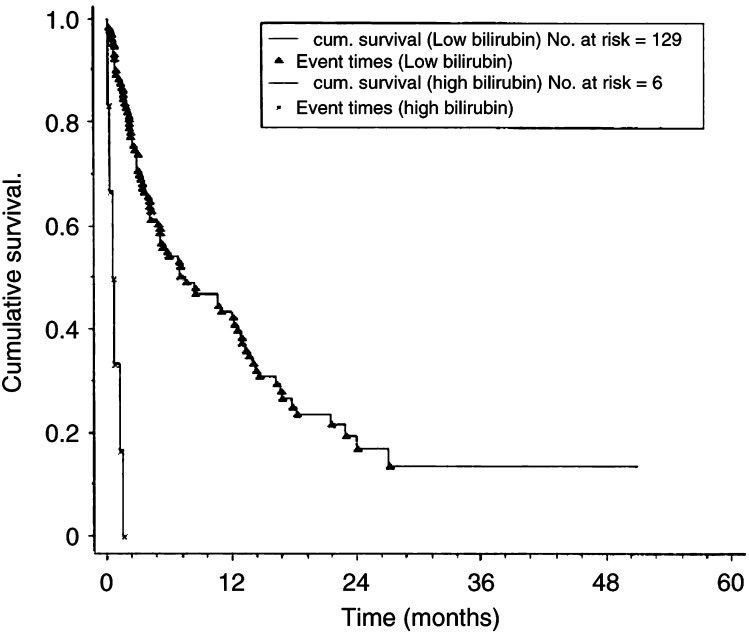
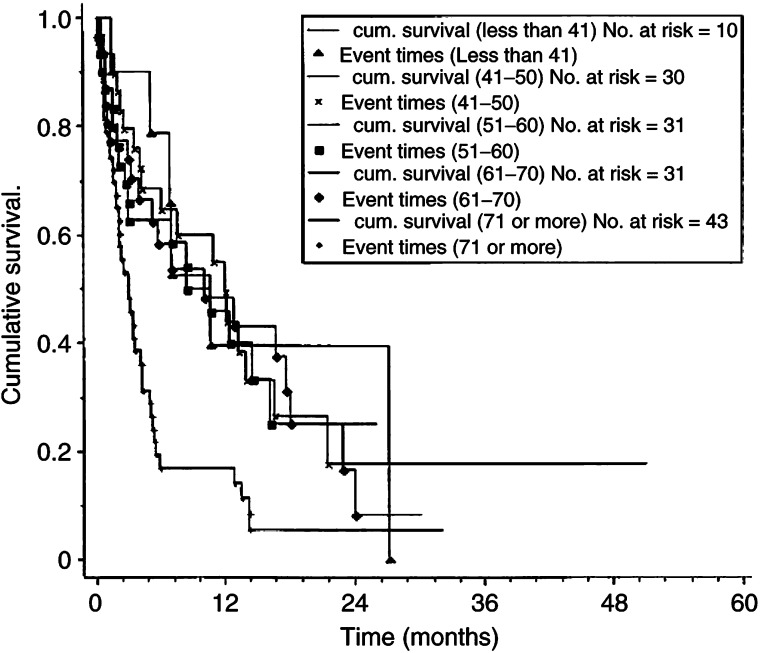
Median survival from liver metastases secondary to breast cancer is only a few months, with very rare 5-year survival. This study reviewed 145 patients with liver metastases from breast cancer to determine factors that may influence survival. Data were analysed using Kaplan-Meier survival curves, univariate and multivariate analysis. Median survival was 4.23 months (range 0.16-51), with a 27.6% 1-year survival. Factors that significantly predicted a poor prognosis on univariate analysis included symptomatic liver disease, deranged liver function tests, the presence of ascites, histological grade 3 disease at primary presentation, advanced age, oestrogen receptor (ER) negative tumours, carcinoembryonic antigen of over 1000 ng ml(-1) and multiple vs single liver metastases. Response to treatment was also a significant predictor of survival with patients responding to chemo- or endocrine therapy surviving for a median of 13 and 13.9 months, respectively. Multivariate analysis of pretreatment variables identified a low albumin, advanced age and ER negativity as independent predictors of poor survival. The time interval between primary and metastatic disease, metastases at extrahepatic sites, histological subtype and nodal stage at primary presentation did not predict prognosis. Awareness of the prognostic implications of the above factors may assist in selecting the most appropriate treatment for these patients.British Journal of Cancer (2003) 89, 284-290. doi:10.1038/sj.bjc.6601038 www.bjcancer.com
Figures
References
-
- British Breast Group (1974) Assessment of response to treatment in advanced breast cancer. Lancet ii: 38–39 - PubMed
-
- Buzdar A (2001) Endocrine therapy in the treatment of metastatic breast cancer. Semin Oncol 28: 291–304 - PubMed
-
- Carey LA, Ewend MG, Sawyer L, Dees EC, Sartor CI, Graham M (2001) Disproportionate CNS relapse after aggressive neo-adjuvant chemotherapy. Abstract. San Antonio Breast Meeting. San Antonio
-
- Cheung KL, Graves CRL, Robertson JFR (2000) Tumour marker measurements in the diagnosis and monitoring of breast cancer. Cancer Treat Rev 26: 91–102 - PubMed
-
- DeAngelis LM, Delattre J-Y, Posner JB (1989) Radiation-induced dementia in patients cured of brain metastases. Neurology 39: 789–796 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
