

Bone-marrow-derived cells contribute to glomerular endothelial repair in experimental glomerulonephritis
- PMID: 12875975
- PMCID: PMC1868209
- DOI: 10.1016/S0002-9440(10)63683-8
Bone-marrow-derived cells contribute to glomerular endothelial repair in experimental glomerulonephritis
Abstract
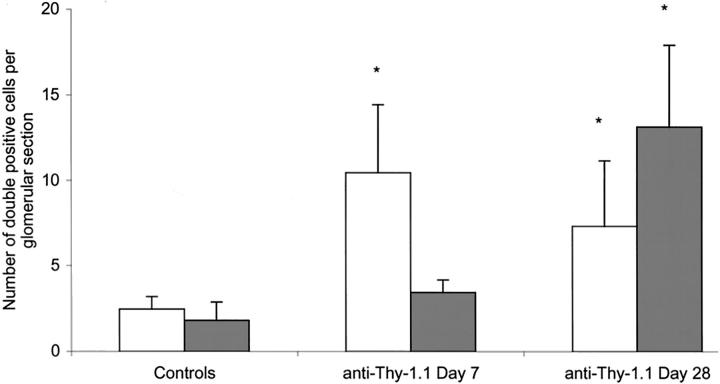
Glomerular endothelial injury plays an important role in the pathogenesis of renal diseases and is centrally involved in renal disease progression. Glomerular endothelial repair may help maintain renal function. We examined whether bone-marrow (BM)-derived cells contribute to glomerular repair. A rat allogenic BM transplant model was used to allow tracing of BM-derived cells using a donor major histocompatibility complex class-I specific mAb. In glomeruli of chimeric rats we identified a small number of donor-BM-derived endothelial and mesangial cells, which increased in a time-dependent manner. Induction of anti-Thy-1.1-glomerulonephritis (transient mesangial and secondary glomerular endothelial injury) caused a significant, more than fourfold increase in the number of BM-derived glomerular endothelial cells at day 7 after anti-Thy-1.1 injection compared to chimeric rats without glomerular injury. The level of BM-derived endothelial cells remained high at day 28. We also observed a more than sevenfold increase in the number of BM-derived mesangial cells at day 28. BM-derived endothelial and mesangial cells were fully integrated in the glomerular structure. Our data show that BM-derived cells participate in glomerular endothelial and mesangial cell turnover and contribute to microvascular repair. These findings provide novel insights into the pathogenesis of renal disease and suggest a potential role for stem cell therapy.
Figures





References
-
- Kang DH, Kanellis J, Hugo C, Truong L, Anderson S, Kerjaschki D, Schreiner GF, Johnson RJ: Role of the microvascular endothelium in progressive renal disease. J Am Soc Nephrol 2002, 13:806-816 - PubMed
-
- Yamanaka N, Shimizu A: Role of glomerular endothelial damage in progressive renal disease. Kidney Blood Press Res 1999, 22:13-20 - PubMed
-
- Abouna GM, Al Adnani MS, Kremer GD, Kumar SA, Daddah SK, Kusma G: Reversal of diabetic nephropathy in human cadaveric kidneys after transplantation into non-diabetic recipients. Lancet 1983, 2:1274-1276 - PubMed
-
- Clark G, White RH, Glasgow EF, Chantler C, Cameron JS, Gill D, Comley LA: Poststreptococcal glomerulonephritis in children: clinicopathological correlations and long-term prognosis. Pediatr Nephrol 1988, 2:381-388 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
