

Pathology and pathogenesis of bioterrorism-related inhalational anthrax
- PMID: 12875989
- PMCID: PMC1868222
- DOI: 10.1016/S0002-9440(10)63697-8
Pathology and pathogenesis of bioterrorism-related inhalational anthrax
Abstract
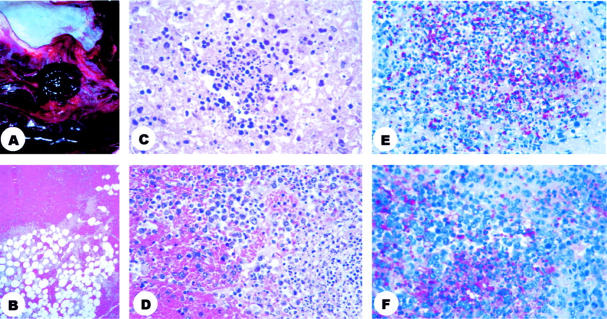
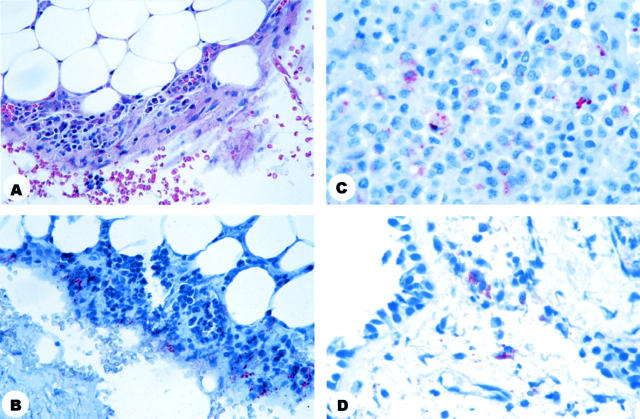
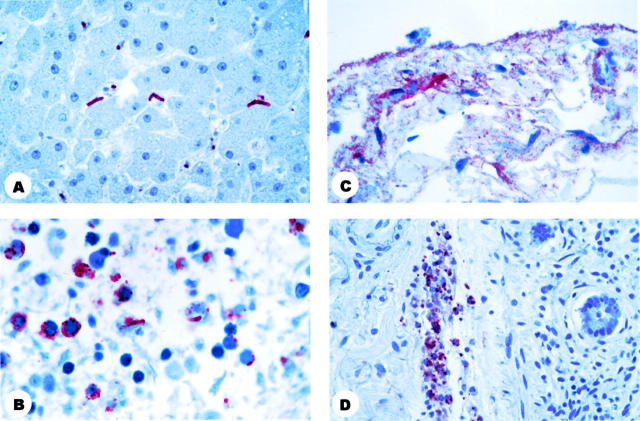
During October and November 2001, public health authorities investigated 11 patients with inhalational anthrax related to a bioterrorism attack in the United States. Formalin-fixed samples from 8 patients were available for pathological and immunohistochemical (IHC) study using monoclonal antibodies against the Bacillus anthracis cell wall and capsule. Prominent serosanguinous pleural effusions and hemorrhagic mediastinitis were found in 5 patients who died. Pulmonary infiltrates seen on chest radiographs corresponded to intraalveolar edema and hyaline membranes. IHC assays demonstrated abundant intra- and extracellular bacilli, bacillary fragments, and granular antigen-staining in mediastinal lymph nodes, surrounding soft tissues, and pleura. IHC staining in lung, liver, spleen, and intestine was present primarily inside blood vessels and sinusoids. Gram's staining of tissues was not consistently positive. In 3 surviving patients, IHC of pleural samples demonstrated abundant granular antigen-staining and rare bacilli while transbronchial biopsies showed granular antigen-staining in interstitial cells. In surviving patients, bacilli were not observed with gram's stains. Pathological and IHC studies of patients who died of bioterrorism-related inhalational anthrax confirmed the route of infection. IHC was indispensable for diagnosis of surviving anthrax cases. The presence of B. anthracis antigens in the pleurae could explain the prominent and persistent hemorrhagic pleural effusions.
Figures

Comment in
-
Exposing a killer: pathologists angle for anthrax.Am J Pathol. 2003 Nov;163(5):1699-702. doi: 10.1016/S0002-9440(10)63526-2. Am J Pathol. 2003. PMID: 14578167 Free PMC article. Review. No abstract available.
References
-
- CDC Update: investigation of anthrax associated with intentional exposure and interim public health guidelines, October 2001. MMWR Morb Mortal Wkly Rep 2001, 50:889-893 - PubMed
-
- CDC Update: investigation of bioterrorism-related anthrax and interim guidelines for exposure management and antimicrobial therapy, October 2001. MMWR Morb Mortal Wkly Rep 2001, 50:909-919 - PubMed
-
- CDC Update: investigation of bioterrorism-related anthrax and interim guidelines for clinical evaluation of persons with possible anthrax. MMWR Morb Mortal Wkly Rep 2001, 50:941-948 - PubMed
-
- CDC Update: investigation of bioterrorism-related anthrax and adverse events from antimicrobial prophylaxis. MMWR Morb Mortal Wkly Rep 2001, 50:973-976 - PubMed
-
- CDC Update: Investigation of bioterrorism-related inhalational anthrax, Connecticut, 2001. MMWR Morb Mortal Wkly Rep 2001, 50:1029-1031 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
