

Congenital longitudinal deficiency of the tibia
- PMID: 12879290
- PMCID: PMC3461877
- DOI: 10.1007/s00264-003-0490-5
Congenital longitudinal deficiency of the tibia
Abstract
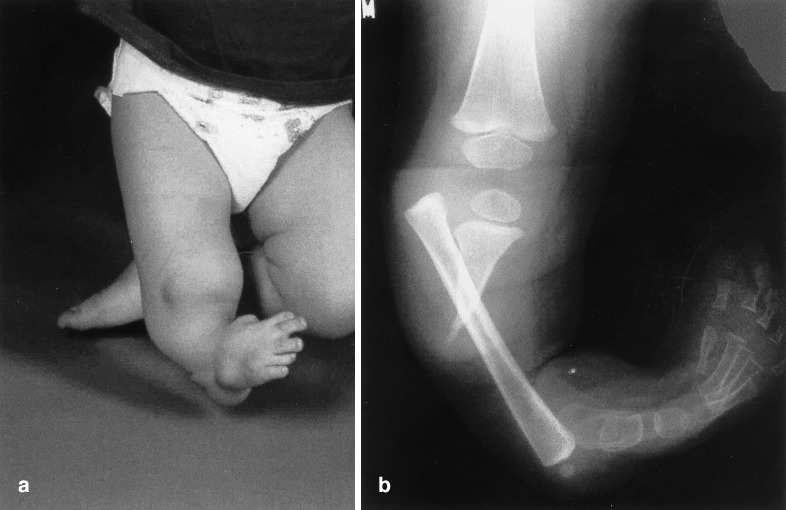
We performed a clinical and radiographic review of 15 patients (19 limbs) with longitudinal deficiency of the tibia treated between 1981 and 2001. Ten limbs with Kalamchi type I deficiencies were managed by through-knee amputation. Five type II deficiencies were treated by foot ablation and tibiofibular synostosis, either at the same time or staged, but prosthetic problems may arise from varus alignment and prominence of the proximal fibula. Patients with type III deficiencies (four cases) were treated by foot ablation. Prosthetic problems relating to proximal or distal tibiofibular instability may necessitate additional surgical intervention.
Nous avons fait une révision clinique et radiographique de 15 malades (19 membres) présentant une déficience longitudinale du tibia traitée entre 1981 et 2001. Dix membres avec un déficit type Kalamchi type I ont été traités par une désarticulation du genou. Cinq type II ont été traités par ablation du pied et synostose tibiofibulaire, en un ou plusieurs temps, mais, dans ces cas des problèmes prothétiques peuvent survenir à cause d'un varus ou de la proéminence du péroné proximal. Les malades avec un type III (quatre cas) a été traité par l'ablation du pied. Les problèmes prothétiques en relation avec une instabilité tibiofibulaire proximale ou distale peuvent nécessiter une intervention chirurgicale supplémentaire.
Figures

References
-
- Brown FW (1965) Construction of a knee joint in congenital total absence of the tibia (Paraxial tibial hemimelia). A preliminary report. J Bone Joint Surg [Am] 47:695–704 - PubMed
-
- Brown FW, Pohnert WH (1972) Construction of a knee joint in meromelia tibia (Congenital absence of the tibia) A fifteen-year followup study. J Bone Joint Surg [Am] 54:1333
-
- Carranza-Bencano Foot Ankle. 1999;20:392. - PubMed
-
- Christini J Pediatr Orthop. 1993;13:378. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
