

Visual outcomes and amblyogenic risk factors in craniosynostotic syndromes: a review of 141 cases
- PMID: 12881344
- PMCID: PMC1771801
- DOI: 10.1136/bjo.87.8.999
Visual outcomes and amblyogenic risk factors in craniosynostotic syndromes: a review of 141 cases
Abstract
Aims: To determine the visual outcome and prevalence of amblyogenic risk factors in children with craniosynostotic syndromes.
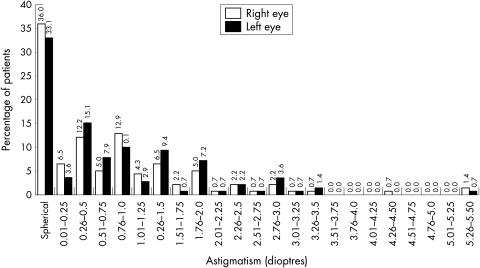
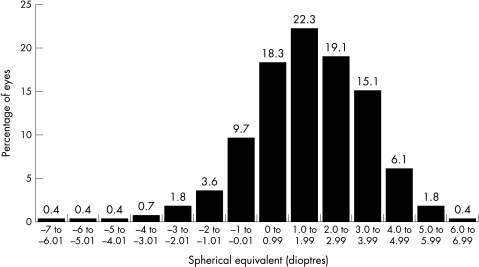
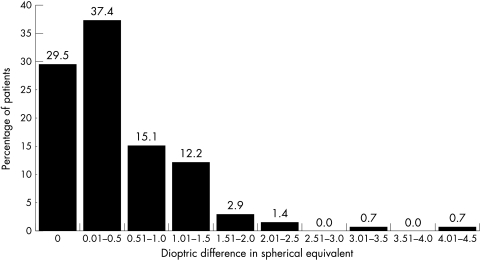
Methods: The case notes of 141 children seen within the craniofacial unit were reviewed and information retrieved on date of birth, age at first and last examination, cycloplegic refraction at last visit, best corrected visual acuity at last visit, horizontal ocular deviation in primary position at first visit, and alphabet pattern if any. The presence of astigmatism, its magnitude, and orientation of axis were determined.
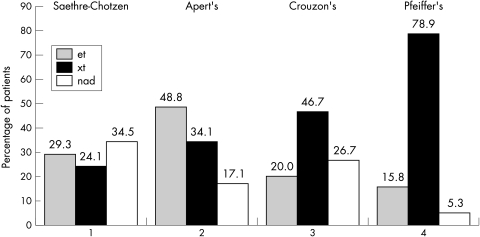
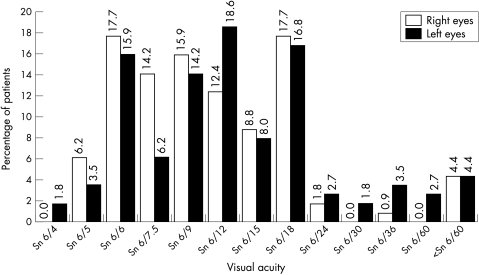
Results: 40.3% of patients had 1 dioptre (D) of astigmatism or greater and, of these, 64% had oblique astigmatism in at least one eye. Anisometropia of 1D or more was found in 18% of patients (age matched normals 3.5%). Horizontal strabismus was found in 70% (38% exotropia, 32% esotropia). Visual outcome results showed 39.8% of patients (45 of 113) had visual acuity of 6/12 or worse in their better eye.
Conclusion: In the largest study to date a poor visual outcome was shown in children with Crouzon's, Pfeiffer's, Apert's, and Saethre-Chotzen syndromes (39.8% with 6/12 or worse in the better eye) together with significant prevalence of amblyogenic risk factors.
Figures
References
-
- Lajeunie E, Le Merrer M, Bonaiti-Pellie C, et al. Genetic study of syndromic coronal craniosynostosis. Am J Med Genet 1995;55:500–4. - PubMed
-
- Steinberger D, Reinhartz T, Unsold R, et al. FGFR2 mutation in clinically non-classifiable autosomal dominant craniosynostosis with pronounced phenotypic variation. Am J Med Genet 1996;66:81–6. - PubMed
-
- Cohen MM Jr. Craniosynostosis: diagnosis, evaluation, and management. New York: Raven, 1996.
-
- Winter RM, Baraitser M. The London dysmorphology database. Oxford: Oxford University Press, 1996.
-
- Katzen JT, McCarthy JG. Syndromes involving craniosynostosis and midface hypoplasia. Otolaryngol Clin N Am 2000;33:1257–84. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical