

Hospital volume, length of stay, and readmission rates in high-risk surgery
- PMID: 12894006
- PMCID: PMC1422689
- DOI: 10.1097/01.SLA.0000081094.66659.c3
Hospital volume, length of stay, and readmission rates in high-risk surgery
Abstract
Objective: Aimed at reducing surgical deaths, several recent initiatives have attempted to establish volume-based referral strategies in high-risk surgery. Although payers are leading the most visible of these efforts, it is unknown whether volume standards will also reduce resource use.
Methods: We studied postoperative length of stay and 30-day readmission rate after 14 cardiovascular and cancer procedures using the 1994-1999 national Medicare database (total n = 2.5 million). We used regression techniques to examine the relationship between length of stay, 30-day readmission, and hospital volume, adjusting for age, gender, race, comorbidity score, admission acuity, and mean social security income.
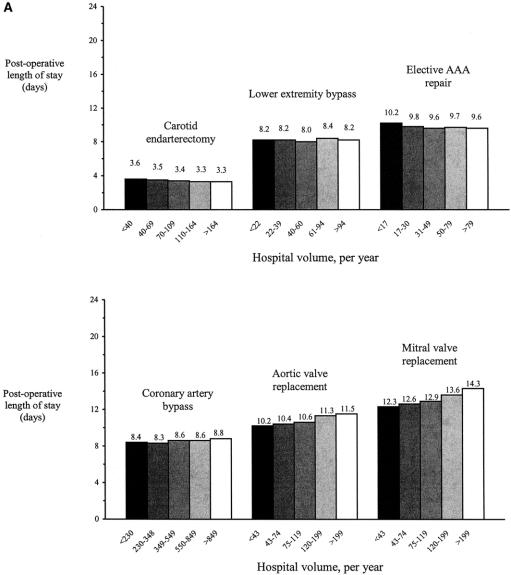
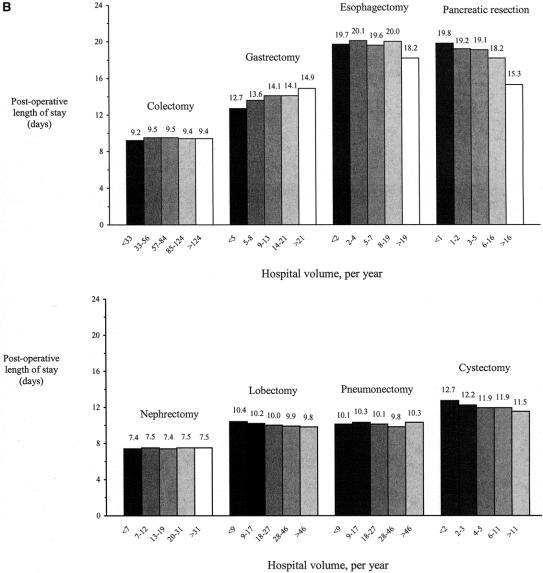
Results: Mean postoperative length of stay ranged from 3.4 days (carotid endarterectomy) to 19.6 days (esophagectomy). There was no consistent relationship between volume and mean length of stay; it significantly increased across volume strata for 7 of the 14 procedures and significantly decreased across volume strata for the other 7. Mean length of stay at very-low-volume and very-high-volume hospitals differed by more than 1 day for 6 procedures. Of these, the mean length of stay was shorter in high-volume hospitals for 3 procedures (pancreatic resection, esophagectomy, cystectomy), but longer for other procedures (aortic and mitral valve replacement, gastrectomy). The 30-day readmission rate also varied widely by procedure, ranging from 9.9% (nephrectomy) to 22.2% (mitral valve replacement). However, volume was not related to 30-day readmission rate with any procedure.
Conclusion: Although hospital volume may be an important predictor of operative mortality, it is not associated with resource use as reflected by length of stay or readmission rates.
Figures
Comment in
-
Is it defensible to use volume standards for purchasing care?Ann Surg. 2003 Aug;238(2):168-9. doi: 10.1097/01.sla.0000081084.36358.2d. Ann Surg. 2003. PMID: 12894007 Free PMC article. No abstract available.
-
Is bigger better? Re-exploring the relationship between hospital volume and surgical outcomes.Gastroenterology. 2004 Mar;126(3):924-6. doi: 10.1053/j.gastro.2003.10.088. Gastroenterology. 2004. PMID: 14988850 No abstract available.
References
-
- Birkmeyer JD, Siewers AE, Finlayson EVA, et al. Hospital volume and surgical mortality in the United States: 1994-1999. N Engl J Med. 2002;346:1128–1137. - PubMed
-
- Begg CB, Cramer LD, Hoskins WJ, et al. Impact of hospital volume on operative mortality for major cancer surgery. JAMA. 1998;280:1747–1751. - PubMed
-
- Dudley RA, Johansen KL, Brand R, et al. Selective referral to high volume hospitals: estimating the potential impact on hospital mortality. JAMA. 2000;283:1159–1166. - PubMed
-
- Halm EA, Lee C, Chassin MR. Is volume related to outcome in health care? A systematic review and methodologic critique of the literature. Ann Intern Med. 2002; 137(6):I52. - PubMed
-
- Birkmeyer JD, Finlayson EV, Birkmeyer CM. Volume standards for high-risk surgical procedures: potential benefits of the Leapfrog initiative. Surgery. 2001;130:415–422. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
