

SARS outbreaks in Ontario, Hong Kong and Singapore: the role of diagnosis and isolation as a control mechanism
- PMID: 12900200
- PMCID: PMC7134599
- DOI: 10.1016/s0022-5193(03)00228-5
SARS outbreaks in Ontario, Hong Kong and Singapore: the role of diagnosis and isolation as a control mechanism
Abstract
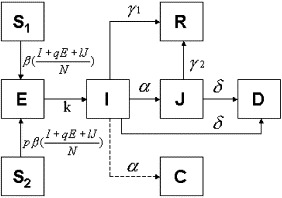
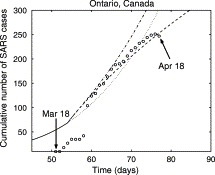
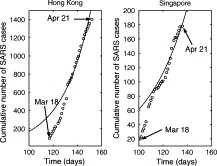
In this article we use global and regional data from the SARS epidemic in conjunction with a model of susceptible, exposed, infective, diagnosed, and recovered classes of people ("SEIJR") to extract average properties and rate constants for those populations. The model is fitted to data from the Ontario (Toronto) in Canada, Hong Kong in China and Singapore outbreaks and predictions are made based on various assumptions and observations, including the current effect of isolating individuals diagnosed with SARS. The epidemic dynamics for Hong Kong and Singapore appear to be different from the dynamics in Toronto, Ontario. Toronto shows a very rapid increase in the number of cases between March 31st and April 6th, followed by a significant slowing in the number of new cases. We explain this as the result of an increase in the diagnostic rate and in the effectiveness of patient isolation after March 26th. Our best estimates are consistent with SARS eventually being contained in Toronto, although the time of containment is sensitive to the parameters in our model. It is shown that despite the empirically modeled heterogeneity in transmission, SARS' average reproductive number is 1.2, a value quite similar to that computed for some strains of influenza (J. Math. Biol. 27 (1989) 233). Although it would not be surprising to see levels of SARS infection higher than 10% in some regions of the world (if unchecked), lack of data and the observed heterogeneity and sensitivity of parameters prevent us from predicting the long-term impact of SARS. The possibility that 10 or more percent of the world population at risk could eventually be infected with the virus in conjunction with a mortality rate of 3-7% or more, and indications of significant improvement in Toronto support the stringent measures that have been taken to isolate diagnosed cases.
Figures

References
-
- Anderson R.M., May R.M. Infectious Diseases of Humans. Oxford University Press; Oxford: 1991.
-
- BBC News, 2003. Ministers may review SARS status. http://news.bbc.co.uk/1/hi/health/2979623.stm, 27th April.
-
- Bradsher, K., 2003a. Carrier of SARS made 7 flights before treatment. The New York Times, 11th April.
-
- Bradsher, K., 2003b. SARS is here to stay, Hong Kong and Singapore tell citizens. The New York Times, 8th April.
-
- Brauer F., Castillo-Chavez C. Mathematical Models in Population Biology and Epidemiology. Springer; New York: 2000.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
