

Hyperuricemia in childhood primary hypertension
- PMID: 12900431
- PMCID: PMC1800942
- DOI: 10.1161/01.HYP.0000085858.66548.59
Hyperuricemia in childhood primary hypertension
Abstract
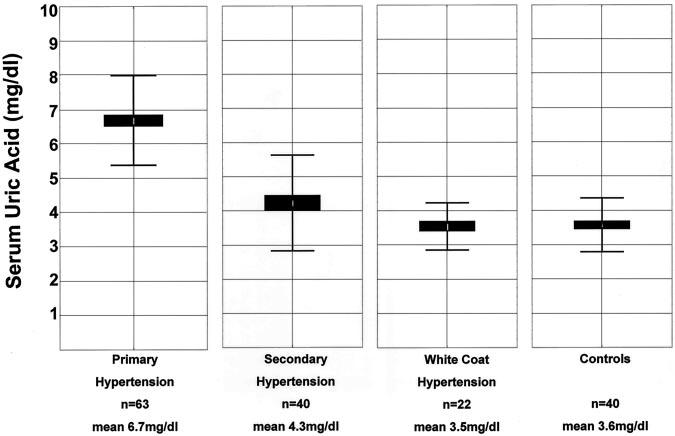
Experimental animal models suggest that uric acid might have a pathogenic role in the early development of primary hypertension. We hypothesized that serum uric acid is correlated with blood pressure in children with new-onset, untreated, primary hypertension. We evaluated 125 consecutive children referred to the Baylor Pediatric Renal Program for evaluation of hypertension. None of the subjects had previously been evaluated or treated for hypertension. The children ranged in age from 6 to 18 years (mean, 13.4+/-3.3) and had normal renal function (creatinine clearance >80 mL x min(-1) x 1.73 m(-2)). Sixty-three children had primary hypertension, 40 had secondary hypertension, and 22 had white-coat hypertension. Forty controls with normal blood pressure were recruited from the renal clinic. Uric acid levels were directly correlated with systolic (r=0.80, P=0.0002) and diastolic (r=0.66, P=0.0006) blood pressure in controls and in subjects with primary hypertension and were independent of renal function. Serum uric acid concentrations >5.5 mg/dL were found in 89% of subjects with primary hypertension, in 30% with secondary hypertension, in 0% with white-coat hypertension, and in 0% of controls. We conclude that serum uric acid is directly correlated with blood pressure in untreated children and that a serum uric acid value >5.5 mg/dL in an adolescent being evaluated for hypertension strongly suggests primary hypertension as opposed to white-coat or secondary hypertension. These results are consistent with the hypothesis that uric acid might have a role in the early pathogenesis of primary hypertension.
Figures


References
-
- Klag MJ, Whelton PK, Randall BL, Neaton JD, Brancati FL, Ford CE, Shulman NB, Stamler J. Blood pressure and end-stage renal disease in men. N Engl J Med. 1996;334:13–18. - PubMed
-
- Coresh J, Wei GL, McQuillan G, Brancati FL, Levey AS, Jones C, Klag MJ. Prevalence of high blood pressure and elevated serum creatinine level in the United States: findings from the third National Health and Nutrition Examination Survey (1988–1994) Arch Intern Med. 2001;161:1207–1216. - PubMed
-
- Mohamed FA. On chronic Bright's disease, and its essential symptoms. Lancet. 1879;1:399–401.
-
- Cannon PJ, Stason WB, Demartini FE, Sommers SC, Laragh JH. Hyper-uricemia in primary and renal hypertension. N Engl J Med. 1966;275:457–464. - PubMed
-
- Kinsey D, Walther R, Sise HS, Whitelaw G, Smithwick R. Incidence of hyperuricemia in 400 hypertensive subjects. Circulation. 1961;24:972–973.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
