

Epidemiology and outcome of nosocomial and community-onset bloodstream infection
- PMID: 12904371
- PMCID: PMC179863
- DOI: 10.1128/JCM.41.8.3655-3660.2003
Epidemiology and outcome of nosocomial and community-onset bloodstream infection
Abstract
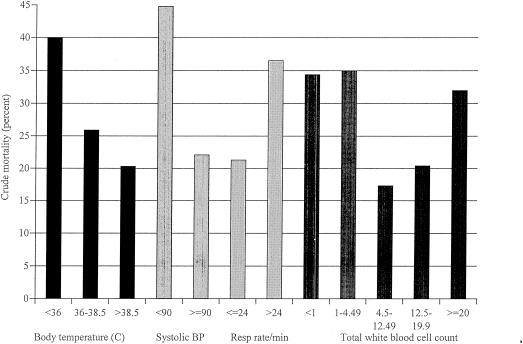
We performed a prospective study of bloodstream infection to determine factors independently associated with mortality. Between February 1999 and July 2000, 929 consecutive episodes of bloodstream infection at two tertiary care centers were studied. An ICD-9-based Charlson Index was used to adjust for underlying illness. Crude mortality was 24% (14% for community-onset versus 34% for nosocomial bloodstream infections). Mortality attributed to the bloodstream infection was 17% overall (10% for community-onset versus 23% for nosocomial bloodstream infections). Multivariate logistic regression revealed the independent associations with in-hospital mortality to be as follows: nosocomial acquisition (odds ratio [OR] 2.6, P < 0.0001), hypotension (OR 2.6, P < 0.0001), absence of a febrile response (P = 0.003), tachypnea (OR 1.9, P = 0.001), leukopenia or leukocytosis (total white blood cell count of <4500 or >20000, P = 0.003), presence of a central venous catheter (OR 2.0, P = 0.0002), and presence of anaerobic organism (OR 2.5, P = 0.04). Even after adjustments were made for underlying illness and length of stay, nosocomial status of bloodstream infection was strongly associated with increased total hospital charges (P < 0.0001). Although accounting for about half of all bloodstream infections, nosocomial bloodstream infections account for most of the mortality and costs associated with bloodstream infection.
Figures
References
-
- Archibald, L., D. Phillips, J. E. Monnet, J. E. McGowan, F. Tenover, and R. Gaynes. 1997. Antimicrobial resistance in isolates from inpatients and outpatients in the United States: increasing importance of the intensive care unit. Clin. Infect. Dis. 24:211-215. - PubMed
-
- Bryant, R. E., A. F. Hood, C. E. Hood, and M. G. Koenig. 1971. Factors affecting mortality of gram-negative rod bacteremia. Arch. Intern. Med. 127:120-128. - PubMed
-
- Centers for Disease Control and Prevention. 2002. Guidelines for the prevention of intravascular catheter-related infections. Morb. Mortal. Wkly. Rep. 51:1-26.
-
- Charlson, M. E., P. Pompei, K. L. Ales, and C. R. MacKenzie. 1987. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40:373-383. - PubMed
-
- Darouiche, R. O., I. Raad, S. O. Heard, J. I. Thornby, O. C. Wenker, A. Gabrielli, J. Berg, N. Khardori, H. Hanna, R. Hachem, R. L. Harris, and G. Mayhall. 1999. A comparison of two antimicrobial-impregnated central venous catheters. N. Engl. J. Med. 340:1-8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
