

Dimensions of patient-provider communication and diabetes self-care in an ethnically diverse population
- PMID: 12911644
- PMCID: PMC1494904
- DOI: 10.1046/j.1525-1497.2003.31968.x
Dimensions of patient-provider communication and diabetes self-care in an ethnically diverse population
Abstract
Background: Patient-provider communication is essential for effective care of diabetes and other chronic illnesses. However, the relative impact of general versus disease-specific communication on self-management is poorly understood, as are the determinants of these 2 communication dimensions.
Design: Cross-sectional survey.
Setting: Three VA heath care systems, 1 county health care system, and 1 university-based health care system.
Patients: Seven hundred fifty-two diabetes patients were enrolled. Fifty-two percent were nonwhite, 18% had less than a high-school education, and 8% were primarily Spanish-speaking.
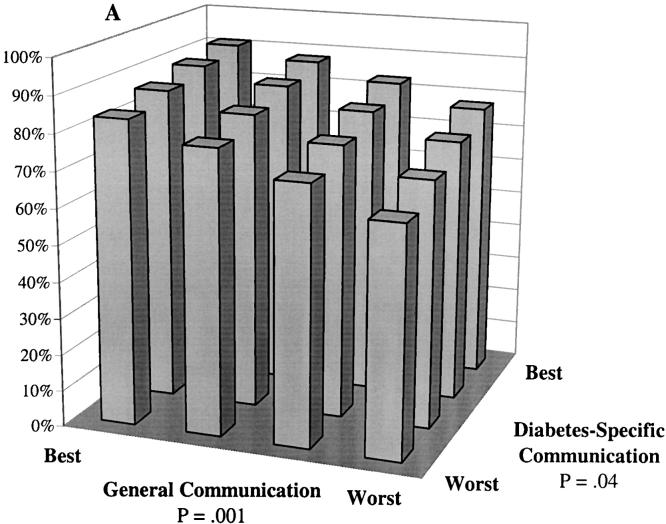
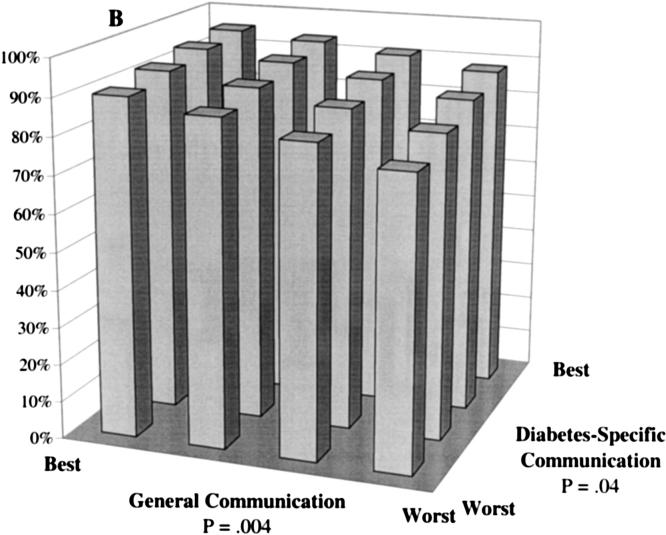
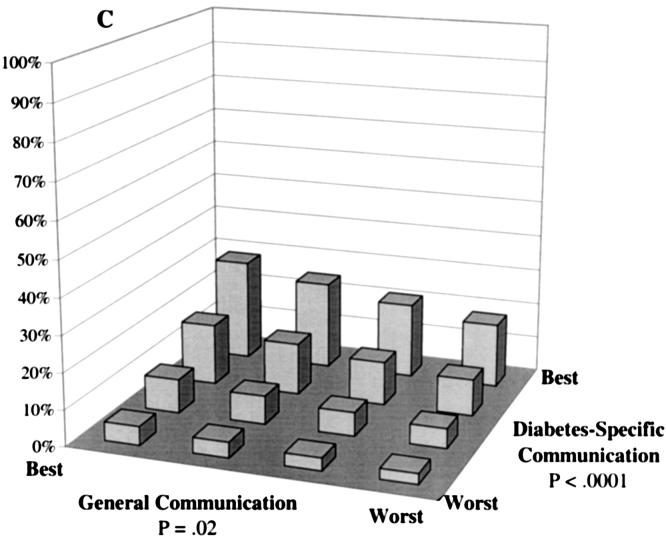
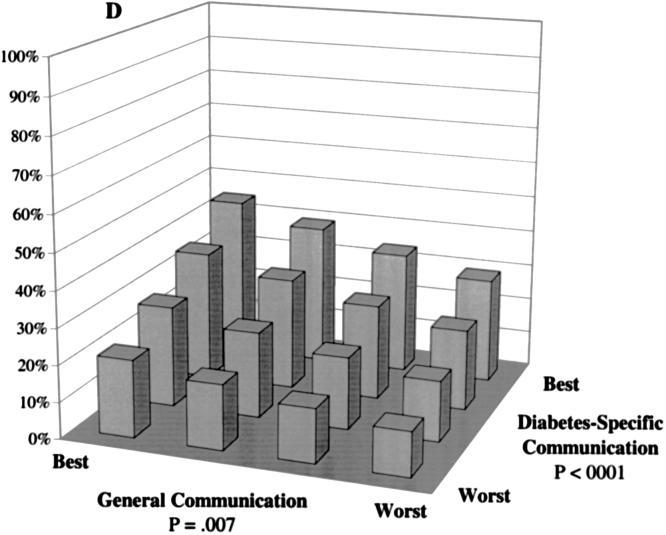
Measurements and main results: Patients' assessments of providers' general and diabetes-specific communication were measured using validated scales. Self-reported foot care; and adherence to hypoglycemic medications, dietary recommendations, and exercise were measured using standard items. General and diabetes-specific communication reports were only moderately correlated (r =.35) and had differing predictors. In multivariate probit analyses, both dimensions of communication were independently associated with self-care in each of the 4 areas examined. Sociodemographically vulnerable patients (racial and language minorities and those with less education) reported communication that was as good or better than that reported by other patients. Patients receiving most of their diabetes care from their primary provider and patients with a longer primary care relationship reported better general communication. VA and county clinic patients reported better diabetes-specific communication than did university clinic patients.
Conclusions: General and diabetes-specific communication are related but unique facets of patient-provider interactions, and improving either one may improve self-management. Providers in these sites are communicating successfully with vulnerable patients. These findings reinforce the potential importance of continuity and differences among VA, county, and university health care systems as determinants of patient-provider communication.
Figures
Comment in
-
Research on patient-clinician relationships: celebrating success and identifying the next scope of work.J Gen Intern Med. 2003 Aug;18(8):677-8. doi: 10.1046/j.1525-1497.2003.30615.x. J Gen Intern Med. 2003. PMID: 12911653 Free PMC article. No abstract available.
References
-
- Harris MI. Health care and health status and outcomes for patients with type 2 diabetes. Diabetes Care. 2000;23:754–8. - PubMed
-
- Saaddine JB, Engelgau MM, Beckles GL, Gregg EW, Thompson TJ, Narayan KM. A diabetes report card for the United States: quality of care in the 1990s. Ann Intern Med. 2002;136:565–74. - PubMed
-
- Glasgow RE, Anderson RM. In diabetes care, moving from compliance to adherence is not enough. Something entirely different is needed. Diabetes Care. 1999;22:2090–2. - PubMed
-
- Anderson RM, Funnell MM. Compliance and adherence are dysfunctional concepts in diabetes care. Diabetes Educ. 2000;26:597–604. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical