

Medical errors related to discontinuity of care from an inpatient to an outpatient setting
- PMID: 12911647
- PMCID: PMC1494907
- DOI: 10.1046/j.1525-1497.2003.20722.x
Medical errors related to discontinuity of care from an inpatient to an outpatient setting
Abstract
Objective: To determine the prevalence of medical errors related to the discontinuity of care from an inpatient to an outpatient setting, and to determine if there is an association between these medical errors and adverse outcomes.
Patients: Eighty-six patients who had been hospitalized on the medicine service at a large academic medical center and who were subsequently seen by their primary care physicians at the affiliated outpatient practice within 2 months after discharge.
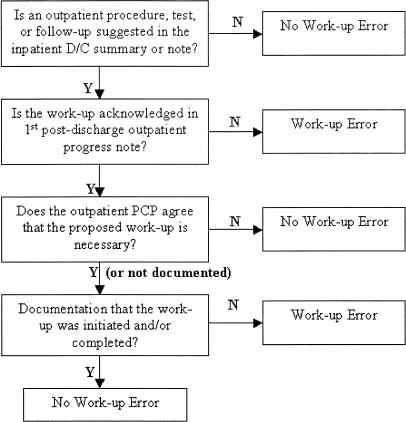
Design: Each patient's inpatient and outpatient medical record was reviewed for the presence of 3 types of errors related to the discontinuity of care from the inpatient to the outpatient setting: medication continuity errors, test follow-up errors, and work-up errors.
Measurements: Rehospitalizations within 3 months after the initial postdischarge outpatient primary care visit.
Main results: Forty-nine percent of patients experienced at least 1 medical error. Patients with a work-up error were 6.2 times (95%confidence interval [95% CI], 1.3 to 30.3) more likely to be rehospitalized within 3 months after the first outpatient visit. We did not find a statistically significant association between medication continuity errors (odds ratio [OR], 2.5; 95%CI, 0.7 to 8.8) and test follow-up errors (OR, 2.4; 95%CI, 0.3 to 17.1) with rehospitalizations.
Conclusion: We conclude that the prevalence of medical errors related to the discontinuity of care from the inpatient to the outpatient setting is high and may be associated with an increased risk of rehospitalization.
Figures


Comment in
-
Seeing error through new lenses.J Gen Intern Med. 2003 Aug;18(8):675-6. doi: 10.1046/j.1525-1497.2003.30614.x. J Gen Intern Med. 2003. PMID: 12911652 Free PMC article. No abstract available.
References
-
- Petersen LA, Brennan TA, O'Neil AC, Cook EF, Lee TH. Does housestaff discontinuity of care increase the risk for preventable adverse events? Ann Intern Med. 1994;121:866–72. - PubMed
-
- Petersen LA, Orav EJ, Teich JM, O'Neil AC, Brennan TA. Using a computerized sign-out program to improve continuity of inpatient care and prevent adverse events. Jt Comm J Qual Improv. 1998;24:77–87. - PubMed
-
- Kohn LT, Corrigan JM, Donaldson MS. To Err is Human: Building a Safer Health System. Washington, DC: Institute of Medicine, National Academy Press; 2000. - PubMed
-
- Wilson S, Ruscoe W, Chapman M, Miller R. General practitioner-hospital communications: a review of discharge summaries. J Qual Clin Pract. 2001;21:104–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical