

Conventional and molecular epidemiology of tuberculosis in Manitoba
- PMID: 12917019
- PMCID: PMC194617
- DOI: 10.1186/1471-2334-3-18
Conventional and molecular epidemiology of tuberculosis in Manitoba
Abstract
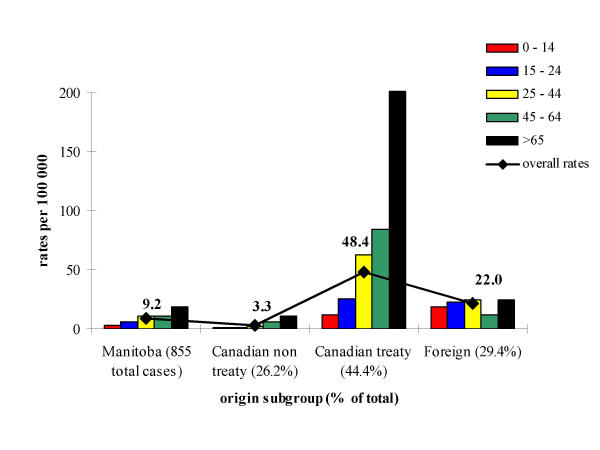
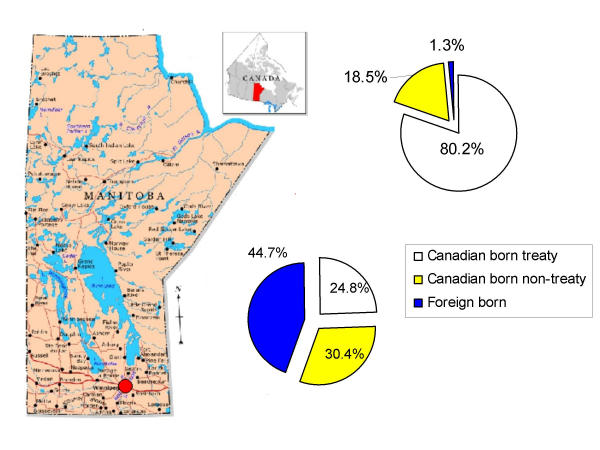
Background: To describe the demographic and geographic distribution of tuberculosis (TB) in Manitoba, thus determining risk factors associated with clustering and higher incidence rates in distinct subpopulations.
Methods: Data from the Manitoba TB Registry was compiled to generate a database on 855 patients with tuberculosis and their contacts from 1992-1999. Recovered isolates of M. tuberculosis were typed by IS6110 restriction fragment length polymorphisms. Bivariate and multivariate logistic regression models were used to identify risk factors involved in clustering.
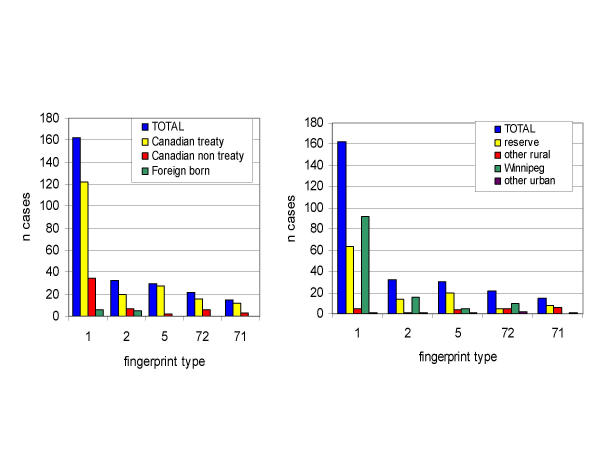
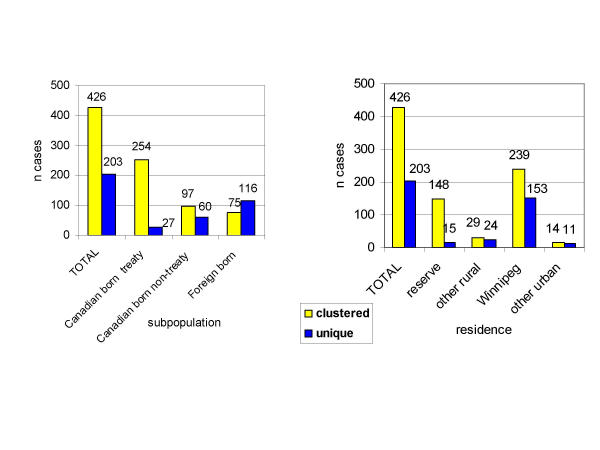
Results: A trend to clustering was observed among the Canadian-born treaty Aboriginal subgroup in contrast to the foreign-born. The dominant type, designated fingerprint type 1, accounts for 25.8% of total cases and 75.3% of treaty Aboriginal cases. Among type 1 patients residing in urban areas, 98.9% lived in Winnipeg. In rural areas, 92.8% lived on Aboriginal reserves. Statistical models revealed that significant risk factors for acquiring clustered tuberculosis are gender, age, ethnic origin and residence. Those at increased risk are: males (p < 0.05); those under age 65 (p < 0.01 for each age subgroup); treaty Aboriginals (p < 0.001), and those living on reserve land (p < 0.001).
Conclusion: Molecular typing of isolates in conjunction with contact tracing data supports the notion of the largest ongoing transmission of a single strain of TB within the treaty-status population of Canada recorded to date. This data demonstrates the necessity of continued surveillance of countries with low prevalence of the disease in order to determine and target high-risk populations for concentrated prevention and control measures.
Figures
References
-
- Piheu JA. Tuberculosis 2000: problems and solutions. Int J Tuberc Lung Dis. 1998;2:696–703. - PubMed
-
- Wherret GJ. Tuberculosis in Canada. Ottawa: Royal Commission on Health Services. 1964.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
