

Central skull base osteomyelitis in patients without otitis externa: imaging findings
- PMID: 12917118
- PMCID: PMC7973651
Central skull base osteomyelitis in patients without otitis externa: imaging findings
Abstract
Background and purpose: Skull base osteomyelitis typically arises as a complication of ear infection in older diabetic patients, involves the temporal bone, and has Pseudomonas aeruginosa as the usual pathogen. Atypical skull base osteomyelitis arising from the sphenoid or occipital bones without associated external otitis occurs much less frequently and initially may have headache as the only symptom. The purpose of this study was to review the clinical and MR imaging features of central skull base osteomyelitis.
Methods: We retrospectively reviewed MR images obtained in six patients with central skull base osteomyelitis. No patient had predisposing external otitis or osteomyelitis of the temporal bone.
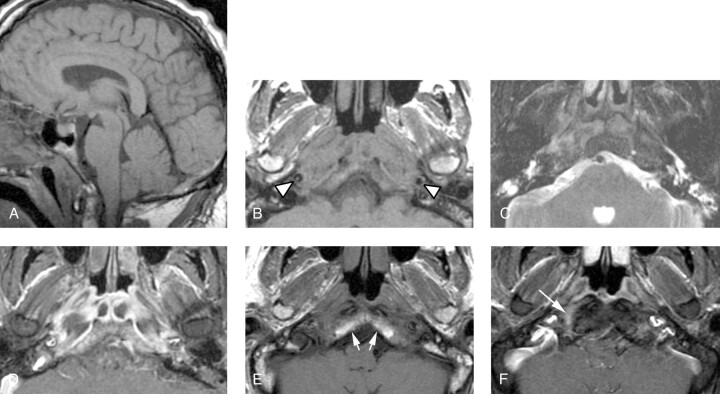
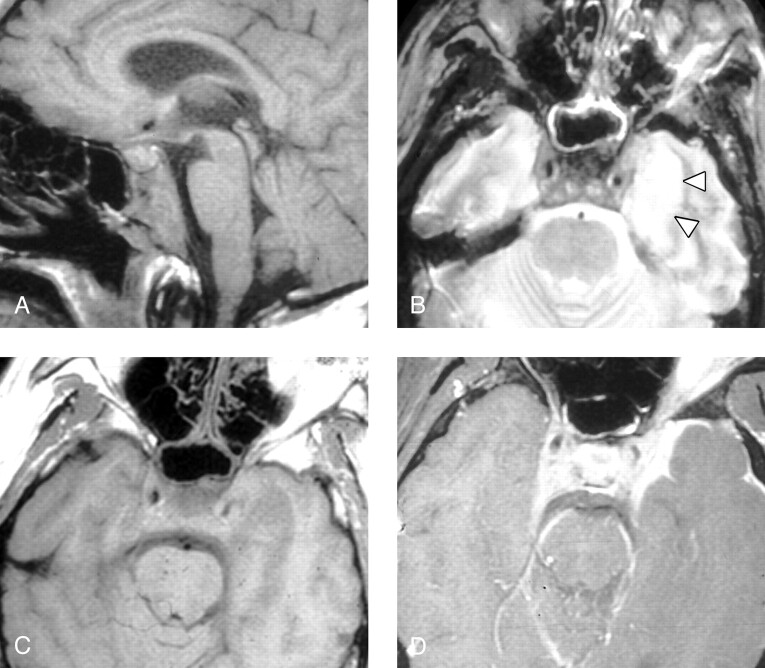
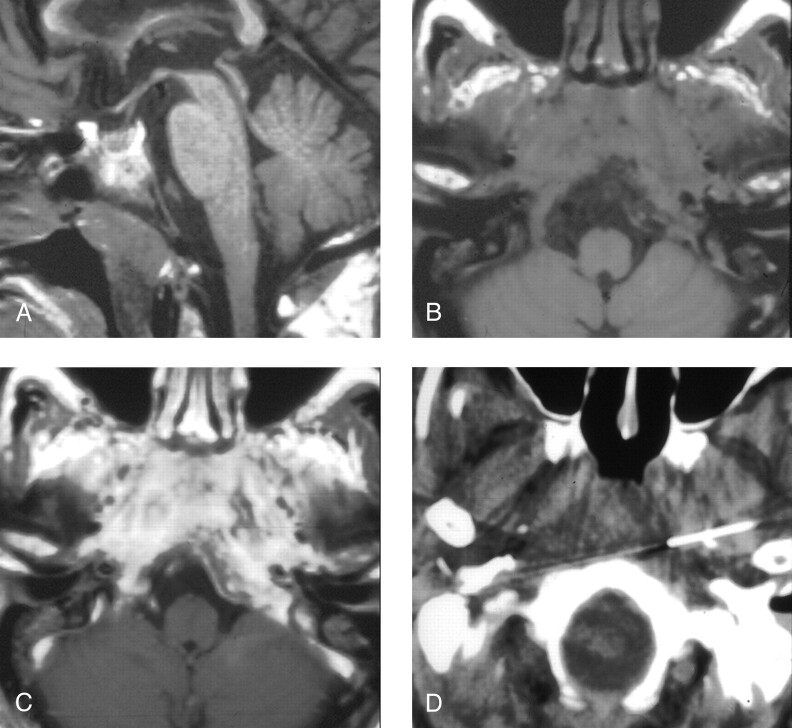
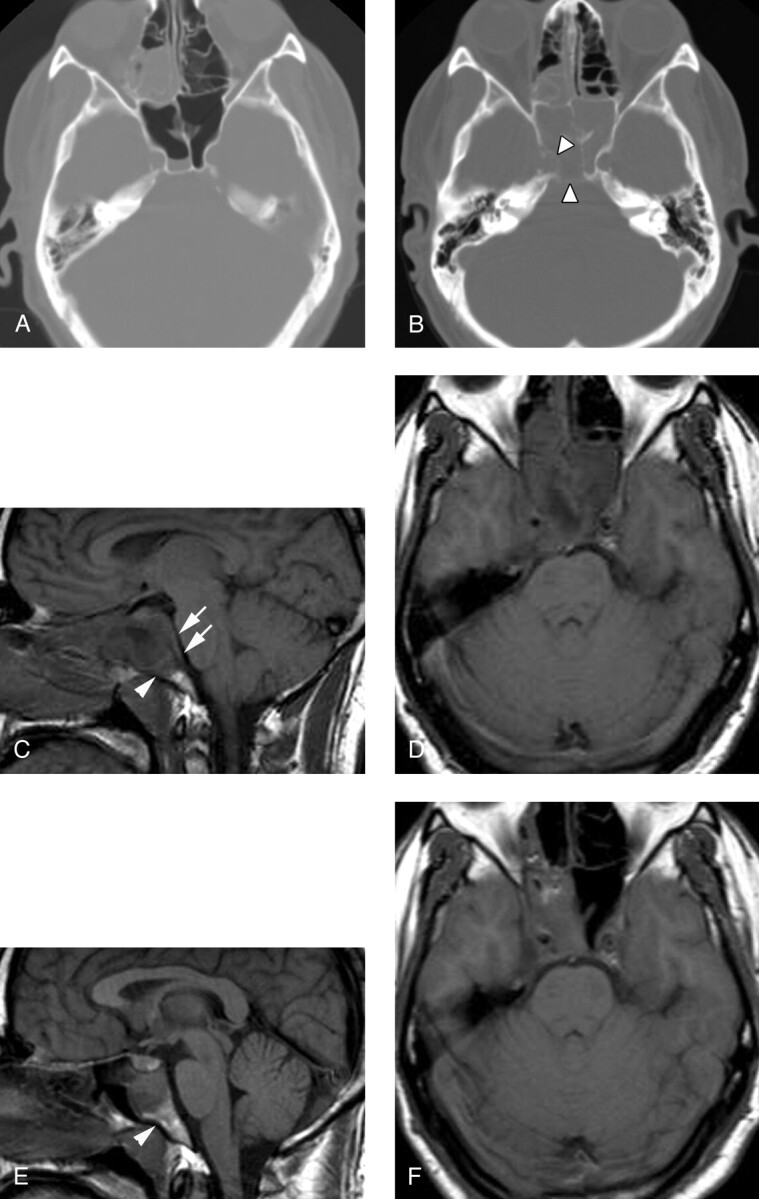
Results: All of our patients presented with headache, no external ear pain, and cranial nerve deficits. Five of six patients had a predisposition to infection, and the erythrocyte sedimentation rate was elevated in the five patients in whom it was checked. In each case, the diagnosis was delayed until MR imaging demonstrated central skull base abnormality, and the diagnosis was then confirmed with tissue sampling. The most consistent imaging findings were clival bone marrow T1 hypointensity and preclival soft tissue infiltration. Five of six patients were cured with no recurrence of skull base infection over a 2-4-year follow-up period.
Conclusion: In the setting of headache, cranial neuropathy, elevated erythrocyte sedimentation rate, and abnormal clival imaging findings, central skull base osteomyelitis should be considered as the likely diagnosis. Early tissue sampling and appropriate treatment may prevent or limit further complications such as intracranial extension, empyema, or death.
Figures
Similar articles
-
Central skull base osteomyelitis as a complication of necrotizing otitis externa: Imaging findings, complications, and challenges of diagnosis.Clin Radiol. 2012 Oct;67(10):e7-e16. doi: 10.1016/j.crad.2012.02.004. Epub 2012 Apr 7. Clin Radiol. 2012. PMID: 22483946 Review.
-
[Atypical osteomyelitis of the base of the skull and malignant otitis externa].Ann Radiol (Paris). 1992;35(6):494-9. Ann Radiol (Paris). 1992. PMID: 1300094 French.
-
[Atypical skull base osteomyelitis suspected of spreading inflammation from the ear canal with unilateral multiple cranial neuropathy and cerebral infarctions].Rinsho Shinkeigaku. 2019 Apr 25;59(4):205-210. doi: 10.5692/clinicalneurol.cn-001258. Epub 2019 Mar 30. Rinsho Shinkeigaku. 2019. PMID: 30930369 Japanese.
-
[Osteomyelitis of the skull base due to otologic or sinus infections. 5 cases].Ann Otolaryngol Chir Cervicofac. 2007 Mar;124(1):25-32. doi: 10.1016/j.aorl.2006.11.001. Ann Otolaryngol Chir Cervicofac. 2007. PMID: 17307132 French.
-
Skull base osteomyelitis secondary to malignant otitis externa.Curr Opin Otolaryngol Head Neck Surg. 2003 Oct;11(5):316-23. doi: 10.1097/00020840-200310000-00002. Curr Opin Otolaryngol Head Neck Surg. 2003. PMID: 14502060 Review.
Cited by
-
Extensive skull base osteomyelitis found radiologically after resolution of otitis externa.BMJ Case Rep. 2020 Aug 24;13(8):e237508. doi: 10.1136/bcr-2020-237508. BMJ Case Rep. 2020. PMID: 32843393 Free PMC article. No abstract available.
-
Diffusion MR imaging features of skull base osteomyelitis compared with skull base malignancy.AJNR Am J Neuroradiol. 2011 Jan;32(1):179-84. doi: 10.3174/ajnr.A2237. Epub 2010 Oct 14. AJNR Am J Neuroradiol. 2011. PMID: 20947640 Free PMC article.
-
Advanced Imaging Techniques in Skull Base Osteomyelitis Due to Malignant Otitis Externa.Curr Radiol Rep. 2018;6(1):3. doi: 10.1007/s40134-018-0263-y. Epub 2018 Jan 22. Curr Radiol Rep. 2018. PMID: 29416952 Free PMC article. Review.
-
Utility of (99m)Tc-MDP hybrid SPECT-CT for diagnosis of skull base osteomyelitis: comparison with planar bone scintigraphy, SPECT, and CT.Jpn J Radiol. 2013 Feb;31(2):81-8. doi: 10.1007/s11604-012-0148-6. Epub 2012 Oct 12. Jpn J Radiol. 2013. PMID: 23065490
-
Osteomyelitis of the craniofacial skeleton.Semin Plast Surg. 2009 May;23(2):73-9. doi: 10.1055/s-0029-1214159. Semin Plast Surg. 2009. PMID: 20567729 Free PMC article.
References
-
- Chandler JR, Grobman L, Quencer R, Serafini A. Osteomyelitis of the base of the skull. Laryngoscope 1986;96:245–251 - PubMed
-
- Mendez G, Jr., Quencer RM, Post MJ, Stokes NA. Malignant external otitis: a radiographic-clinical correlation. AJR Am J Roentgenol 1979;132:957–961 - PubMed
-
- Grobman LR, Ganz W, Casiano R, Goldberg S. Atypical osteomyelitis of the skull base. Laryngoscope 1989;99:671–676 - PubMed
-
- Kimura F, Kim KS, Friedman H, et al. MR imaging of the normal and abnormal clivus. AJR Am J Roentgenol 1990;155:1285–1291 - PubMed
-
- Erdman WA, Tamburro F, Jayson HT, et al. Osteomyelitis: characteristics and pitfalls of diagnosis with MR imaging. Radiology 1991;180:533–539 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources