

Assessment of diffusion and perfusion deficits in patients with small subcortical ischemia
- PMID: 12917127
- PMCID: PMC7973662
Assessment of diffusion and perfusion deficits in patients with small subcortical ischemia
Abstract
Background and purpose: Using perfusion- and diffusion-weighted MR imaging in acute ischemic stroke of the middle cerebral artery (MCA), previous studies have shown a typical pathophysiologic pattern that is characterized by a perfusion deficit larger than the diffusion lesion (mismatch), with the final lesion usually comprising the initial diffusion lesion (core) plus parts of the initial mismatch area. Little is known about underlying pathophysiology in small ischemic stroke. In this study, we used perfusion- and diffusion-weighted MR imaging to investigate the underlying pathophysiology of small subcortical ischemia.
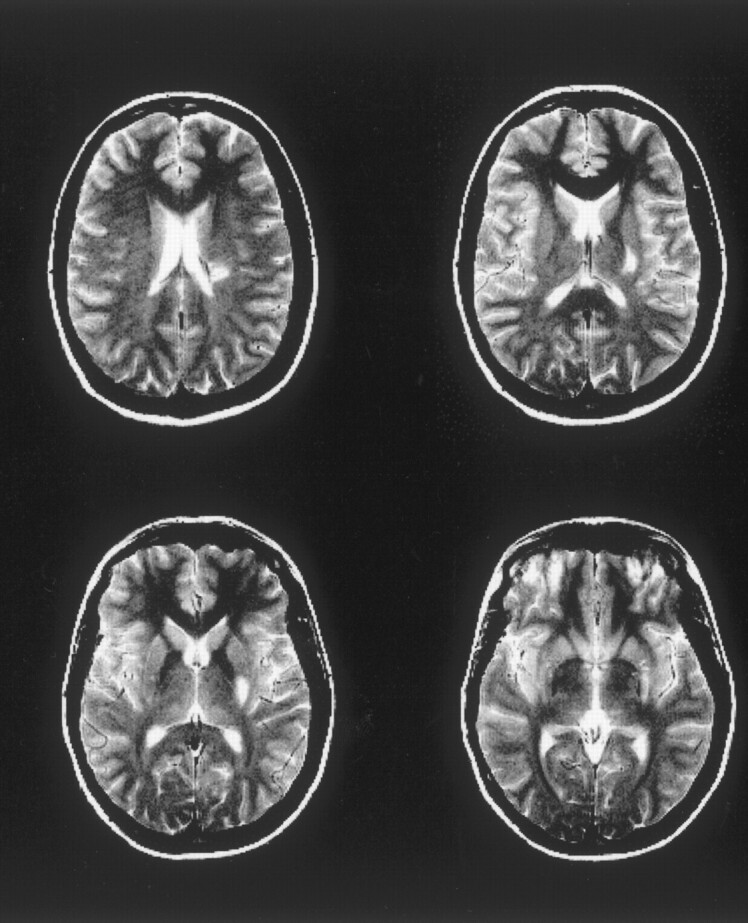
Methods: Six consecutive patients (age range, 42-76 years) with small subcortical ischemia were examined by using a 1.5-T MR system 2-5, 22-55, and 144-392 hours after the onset of symptoms. T2-weighted, diffusion-weighted imaging at b=0 s/mm2 and b=1000 s/mm2, and bolus-track perfusion-weighted imaging were performed. Lesion sizes were determined on the basis of T2-weighted findings as well as those of apparent diffusion coefficient (ADC) maps and CBF.
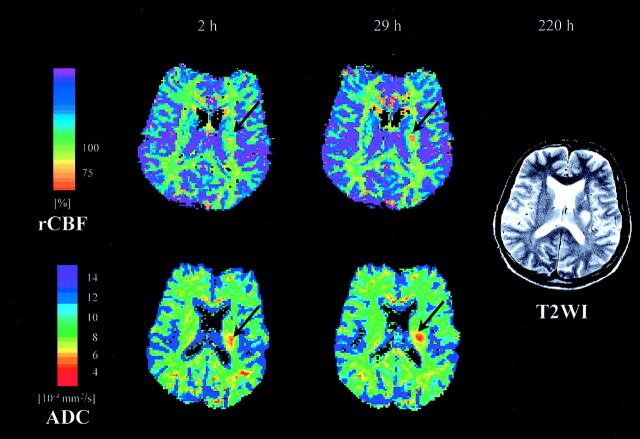
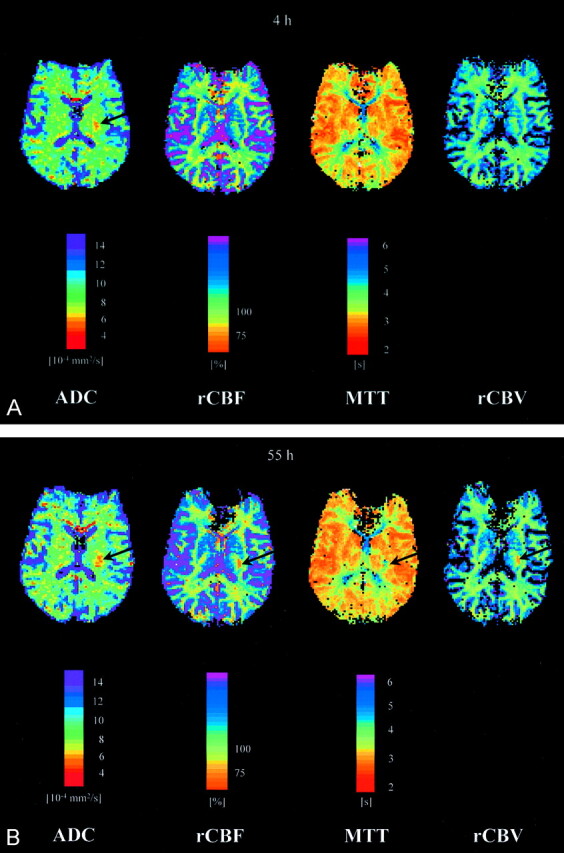
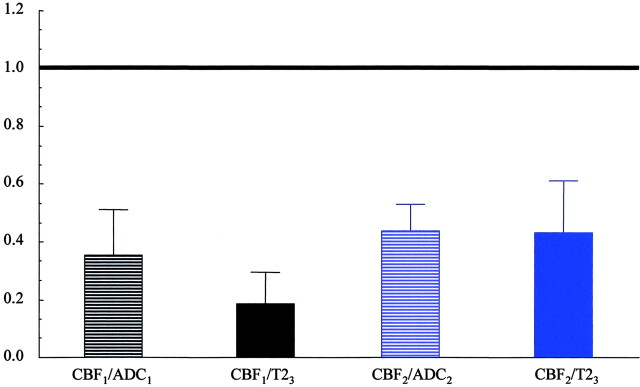
Results: In every patient, the initial CBF lesion was smaller than the initial ADC lesion. Both the CBF lesion and the ADC lesion increased in size from first to second examination. In all instances, however, the CBF lesion remained smaller than the ADC lesion. The CBF lesion observed during the acute phase and the one seen on the following days were both smaller than the final T2 lesion.
Conclusion: Our data suggest that in contrast to previous findings in MCA ischemia in small subcortical infarcts tissue damage may spread beyond the area of the initial perfusion disturbance. In light of the small number of patients, further studies will have to address the relevance of this observation.
Figures
Similar articles
-
Regional ischemia and ischemic injury in patients with acute middle cerebral artery stroke as defined by early diffusion-weighted and perfusion-weighted MRI.Stroke. 1998 May;29(5):939-43. doi: 10.1161/01.str.29.5.939. Stroke. 1998. PMID: 9596239
-
[Application of diffusion-weighted and perfusion magnetic resonance imaging in definition of the ischemic penumbra in hyperacute cerebral infarction].Zhonghua Yi Xue Za Zhi. 2003 Jun 10;83(11):952-7. Zhonghua Yi Xue Za Zhi. 2003. PMID: 12899795 Chinese.
-
Predicting cerebral ischemic infarct volume with diffusion and perfusion MR imaging.AJNR Am J Neuroradiol. 2002 Nov-Dec;23(10):1785-94. AJNR Am J Neuroradiol. 2002. PMID: 12427640 Free PMC article.
-
[The clinical application of diffusion weighted magnetic resonance imaging to acute cerebrovascular disorders].No To Shinkei. 1998 Sep;50(9):787-95. No To Shinkei. 1998. PMID: 9789301 Review. Japanese.
-
Extension of therapeutic window in ischemic stroke by selective mismatch imaging.Int J Stroke. 2019 Jun;14(4):351-358. doi: 10.1177/1747493019840936. Epub 2019 Apr 1. Int J Stroke. 2019. PMID: 30935350 Review.
Cited by
-
Neuroimaging of ischemia and infarction.NeuroRx. 2005 Apr;2(2):265-76. doi: 10.1602/neurorx.2.2.265. NeuroRx. 2005. PMID: 15897950 Free PMC article. Review.
-
Inverse mismatch and lesion growth in small subcortical ischaemic stroke.Eur Radiol. 2010 Dec;20(12):2983-9. doi: 10.1007/s00330-010-1858-8. Epub 2010 Jun 23. Eur Radiol. 2010. PMID: 20571802
-
Association of compromised cerebral perfusion with lenticulostriate artery impairments in the subacute phase of branch atheromatous disease.Ther Adv Neurol Disord. 2022 Jul 4;15:17562864221109746. doi: 10.1177/17562864221109746. eCollection 2022. Ther Adv Neurol Disord. 2022. PMID: 35813607 Free PMC article.
-
Multimodal CT provides improved performance for lacunar infarct detection.AJNR Am J Neuroradiol. 2015 Jun;36(6):1069-75. doi: 10.3174/ajnr.A4255. Epub 2015 Feb 26. AJNR Am J Neuroradiol. 2015. PMID: 25721075 Free PMC article.
-
Perfusion Status in Lacunar Stroke: A Pathophysiological Issue.Diagnostics (Basel). 2023 Jun 8;13(12):2003. doi: 10.3390/diagnostics13122003. Diagnostics (Basel). 2023. PMID: 37370898 Free PMC article. Review.
References
-
- Le Bihan D, Breton E, Lallemand D, et al. MR imaging of intravoxel incoherent motions: application to diffusion and perfusion in neurologic disorders. Radiology 1986;161:401–407 - PubMed
-
- Le Bihan D, Breton E, Lallemand D, et al. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology 1988;168:497–505 - PubMed
-
- Moseley ME, Cohen Y, Mintorovitch J, et al. Early detection of regional cerebral ischemia in cats: comparison of diffusion- and T2-weighted MRI and spectroscopy. Magn Reson Med 1990;14:330–346 - PubMed
-
- Mintorovitch J, Yang GY, Shimizu H, et al. Diffusion-weighted magnetic resonance imaging of acute focal cerebral ischemia: comparison of signal intensity with changes in brain water and Na+, K(+)-ATPase activity. J Cereb Blood Flow Metab 1994;14:332–336 - PubMed
-
- Doege CA, Kerskens CM, Romero BI, et al. MRI of small human stroke shows reversible diffusion changes in subcortical gray matter. Neuroreport 2000;11:2021–2024 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources