

In-hospital morbidity and mortality after endovascular treatment of unruptured intracranial aneurysms in the United States, 1996-2000: effect of hospital and physician volume
- PMID: 12917139
- PMCID: PMC7973658
In-hospital morbidity and mortality after endovascular treatment of unruptured intracranial aneurysms in the United States, 1996-2000: effect of hospital and physician volume
Abstract
Background and purpose: Endovascular therapy is increasingly being used for the treatment of unruptured intracranial aneurysms. Our purpose was to determine the risk of adverse outcomes after contemporary endovascular treatment of unruptured intracranial aneurysms in the United States. Patient, treating physician, and hospital characteristics were tested as potential outcome predictors, with particular attention paid to volume of care.
Methods: We conducted a retrospective cohort study by using the Nationwide Inpatient Sample, 1996-2000. Multivariate logistic and ordinal regressions were used with end points of mortality, discharge other than to home, length of stay, and total hospital charges.
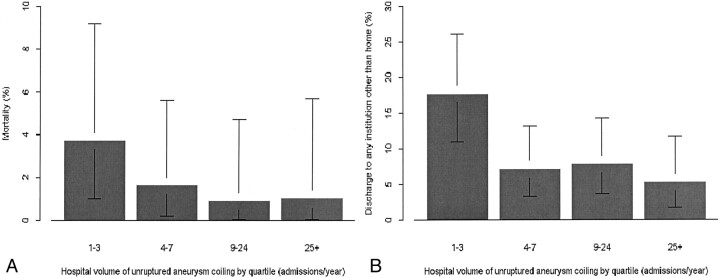
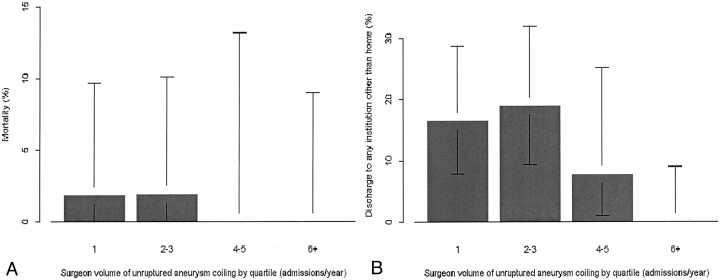
Results: Four hundred twenty-one patients underwent endovascular treatment at 81 hospitals. The in-hospital mortality rate was 1.7%, and 7.6% were discharged to institutions other than home. Analysis was adjusted for age, sex, race, primary payer, year of treatment, and four variables measuring acuity of treatment and medical comorbidity. Median annual number of unruptured aneurysms treated was nine per hospital and three per treating physician. Higher volume hospitals had fewer adverse outcomes; discharge other than to home occurred after 5.2% of operations at high volume hospitals (>23 admissions per year) compared with 17.6% at low volume hospitals (fewer than four admissions per year) (P<.001). Higher physician volume had a similar effect (0% versus 16.4%, P=.03). The mortality rate was lower at high volume hospitals (1.0% versus 3.7%) but not significantly so. At high volume hospitals, length of stay was shorter (P<.001) and total hospital charges were lower (P<.001).
Conclusion: For patients with unruptured aneurysms treated in the United States from 1996 to 2000, endovascular treatment at high volume institutions or by high volume physicians was associated with significantly lower morbidity rates and modestly lower mortality rates. Length of stay was shorter and total hospital charges lower at high volume centers.
Figures
References
-
- Luft HS, Garnick DW, Mark DH, McPhee SJ. Hospital Volume, Physician Volume, and Patient Outcomes. Ann Arbor: Health Administration Press Perspectives;1990
-
- Hewitt M. Interpreting the Volume-Outcome Relationship in the Context of Health Care Quality: Workshop Summary. Washington: National Academy Press;2000
-
- Begg CB, Cramer LD, Hoskins WJ, Brennan MF. Impact of hospital volume on operative mortality for major cancer surgery. JAMA 1998;280:1747–1751 - PubMed
-
- Hillner BE, Smith TJ, Desch CE. Hospital and physician volume or specialization and outcomes in cancer treatment: importance in quality of cancer care. J Clin Oncol 2000;18:2327–2340 - PubMed
-
- Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med 2002;346:1128–1137 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical