

Creatinine clearance and adverse hospital outcomes in patients with acute coronary syndromes: findings from the global registry of acute coronary events (GRACE)
- PMID: 12923009
- PMCID: PMC1767853
- DOI: 10.1136/heart.89.9.1003
Creatinine clearance and adverse hospital outcomes in patients with acute coronary syndromes: findings from the global registry of acute coronary events (GRACE)
Abstract
Objective: To determine whether creatinine clearance at the time of hospital admission is an independent predictor of hospital mortality and adverse outcomes in patients with acute coronary syndromes (ACS).
Design: A prospective multicentre observational study, GRACE (global registry of acute coronary events), of patients with the full spectrum of ACS.
Setting: Ninety four hospitals of varying size and capability in 14 countries across four continents.
Patients: 11 774 patients hospitalised with ACS, including ST and non-ST segment elevation acute myocardial infarction and unstable angina.
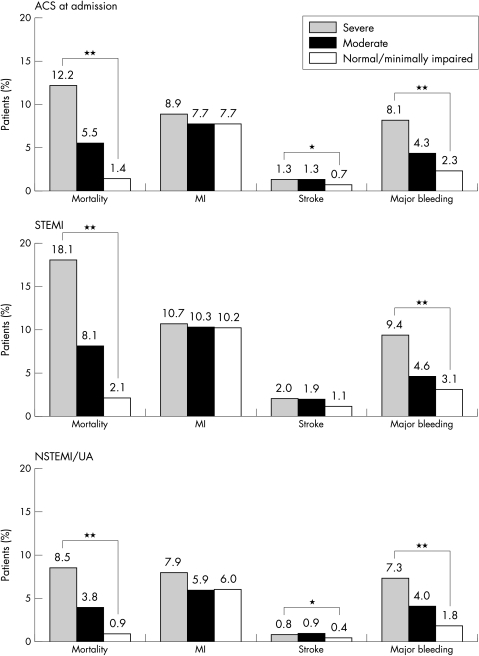
Main outcome measures: Demographic and clinical characteristics, medication use, and in-hospital outcomes were compared for patients with creatinine clearance rates of > 60 ml/min (normal and minimally impaired renal function), 30-60 ml/min (moderate renal dysfunction), and < 30 ml/min (severe renal dysfunction).
Results: Patients with moderate or severe renal dysfunction were older, were more likely to be women, and presented to participating hospitals with more comorbidities than those with normal or minimally impaired renal function. In comparison with patients with normal or minimally impaired renal function, patients with moderate renal dysfunction were twice as likely to die (odds ratio 2.09, 95% confidence interval 1.55 to 2.81) and those with severe renal dysfunction almost four times more likely to die (odds ratio 3.71, 95% confidence interval 2.57 to 5.37) after adjustment for other potentially confounding variables. The risk of major bleeding episodes increased as renal function worsened.
Conclusion: In patients with ACS, creatinine clearance is an important independent predictor of hospital death and major bleeding. These data reinforce the importance of increased surveillance efforts and use of targeted intervention strategies in patients with acute coronary disease complicated by renal dysfunction.
Figures
Comment in
-
Minor renal dysfunction: an emerging independent cardiovascular risk factor.Heart. 2003 Sep;89(9):963-4. doi: 10.1136/heart.89.9.963. Heart. 2003. PMID: 12922986 Free PMC article. No abstract available.
References
-
- Wannamethee SG, Shaper AG, Perry IJ. Serum creatinine concentration and risk of cardiovascular disease: A possible marker for increased risk of stroke. Stroke 1997;28:557–63. - PubMed
-
- Alcorn HG, Wolfson SK Jr, Sutton-Tyrrell K, et al. Risk factors for abdominal aortic aneurysms in older adults enrolled in the cardiovascular health study. Arterioscler Thromb Vasc Biol 1996;16:963–70. - PubMed
-
- Gottlieb SS, Mc Carter RJ, Vogel RA. Effect of beta-blockade on mortality among high risk and low risk patients after myocardial infarction. N Engl J Med 1998;339:489–97. - PubMed
-
- Pahor M, Shorr RI, Somes GW, et al. Diuretic-based treatment and cardiovascular events in patients with mild renal dysfunction enrolled in the systolic hypertension in the elderly program. Arch Intern Med 1998;158:1340–5. - PubMed
-
- Culleton BF, Larson MG, Wilson PW, et al. Cardiovascular disease and mortality in a community-based cohort with mild renal insufficiency. Kidney Int 1999;56:2214–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical