

Apical ballooning of the left ventricle: first series in white patients
- PMID: 12923018
- PMCID: PMC1767823
- DOI: 10.1136/heart.89.9.1027
Apical ballooning of the left ventricle: first series in white patients
Abstract
Background: A cardiac syndrome of "apical ballooning" was recently described, consisting of an acute onset of transient extensive akinesia of the apical and mid portions of the left ventricle, without significant stenosis on the coronary angiogram, accompanied by chest symptoms, ECG changes, and a limited release of cardiac markers disproportionate to the extent of akinesia. Until now, this syndrome has been reported only in Japanese patients.
Objective: To describe 13 white patients who presented with this syndrome over the previous four years.
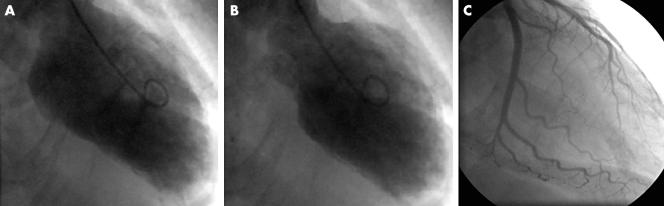
Results: All but one of the patients were women with a mean age of 62 years. Eight of them presented with chest pain, of whom six had cardiogenic shock. In nine patients a triggering factor was identified: emotional stress in three, trauma in one, pneumonia in one, asthma crisis in one, exercise in two, and cerebrovascular accident in one. In all patients left ventriculography showed very extensive apical akinesia ("apical ballooning") in the absence of a significant coronary artery stenosis, not corresponding with the perfusion territory of a single epicardial coronary artery. Mean maximal creatine kinase MB and troponin rise were 27.4 microg/l (range 5.2-115.7 microg/l, median 16.6 microg/l) and 18.7 microg/l (range 2.0-97.6 microg/l, median 14.5 microg/l), respectively. Six patients were treated with intra-aortic balloon counterpulsation. One patient died of multiple organ failure. On necropsy, no myocardial infarction was found. In the 12 survivors, left ventricular systolic function recovered completely within three weeks.
Conclusions: This is the first series of "apical ballooning" to be reported in white patients. Despite dramatic initial presentation, left ventricle function recovered completely within three weeks in the survivors.
Figures
Comment in
-
Apical ballooning of the left ventricle: a distinct entity?Heart. 2003 Sep;89(9):974-6. doi: 10.1136/heart.89.9.974. Heart. 2003. PMID: 12922993 Free PMC article. No abstract available.
References
-
- Tsuchihashi K, Ueshima K, Uchida T, et al. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. J Am Coll Cardiol 2001;38:11–8. - PubMed
-
- Satoh H, Tateishi H, Uchida T, et al. [Takotsubo type cardiomyopathy due to multivessel spasm]. In: Kodama K, Haze K, Hon M, eds. [Clinical aspect of myocardial injury: from ischemia to heart failure] (in Japanese). Tokyo: Kagakuhyouronsya, 1990:56–64.
-
- Dote K, Satoh H, Tateishi H, et al. Myocardial stunning due to simultaneous multivessels spasm: a review of five cases. J Cardiol 1991;21:201–14. - PubMed
-
- Ishihara M, Satoh H, Tateishi H, et al. [“Tako tsubo” type cardiomyopathy] (in Japanese with English abstract). Kokyu to Junkan 1997;45:879–85.
-
- Kawikami H, Matsuoka H, Koyama Y, et al. [“Takotsubo” type cardiomyopathy due to acute myocarditis] (in Japanese with English abstract). Kokyu to Junkan 1998;46:913–7.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous