

Aortic valve and aortic arch pathology after coarctation repair
- PMID: 12923033
- PMCID: PMC1767804
- DOI: 10.1136/heart.89.9.1074
Aortic valve and aortic arch pathology after coarctation repair
Abstract
Objective: To investigate the incidence of clinical problems related to a bicuspid valve (aortic stenosis and regurgitation) and the incidence of ascending aorta and aortic arch pathology in combination with coarctation repair.
Patients: 124 adult patients after surgical correction of aortic coarctation were studied. The incidence of aortic valve, ascending aorta, and aortic arch pathology was determined using echocardiography and magnetic resonance imaging. The median age at coarctation repair was 9 years and at last follow up 28 years.
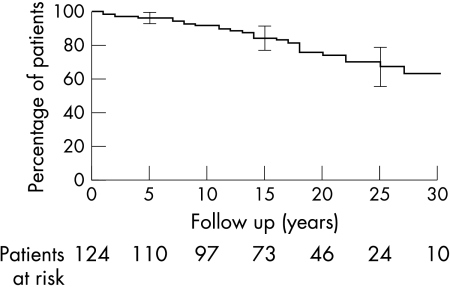
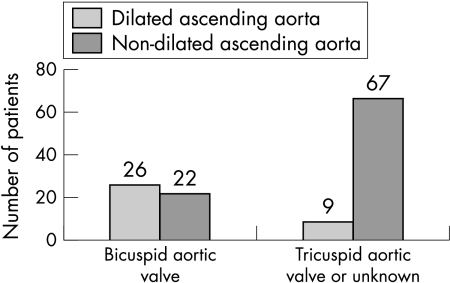
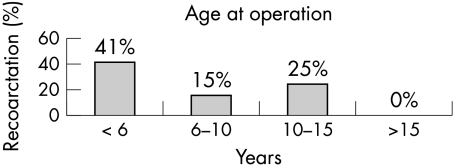
Results: Three patients died from aorta pathology. Aortic valve disease was found in 63% of the patients, requiring an intervention in 22%, at a median of 13 years after coarctation repair. Ascending aorta dilatation was observed in 28% and aortic arch abnormalities in 23%, among whom kinking of the aortic arch was found in 12%. Antihypertensive medication was used in 24%. In the patients with hypertension the age at operation and age at follow up were significantly higher (p = 0.0001 and p < 0.0001, respectively).
Conclusion: In addition to the well known problems of hypertension and recoarctation, aortic valve and aortic arch pathology are commonly encountered in patients with previous coarctation repair. Aortic abnormalities may predispose to dilatation and dissection, thus necessitating careful lifelong attention in all patients with coarctation.
Figures
References
-
- Cohen M, Fuster V, Steele PM, et al. Coarctation of the aorta: long-term follow-up and prediction of outcome after surgical correction. Circulation 1989;80:840–5. - PubMed
-
- Brouwer MH, Kuntze EE, Ebels T, et al. Repair of aortic coarctation in infants. J Thorac Cardiovasc Surg 1991;101:1093–8. - PubMed
-
- Dietl CA, Torres AR, Favaloro RG, et al. Risk of recoarctation in neonates and infants after repair with patch aortoplasty, subclavian flap, and the combined resection-flap procedure. J Thorac Cardiovasc Surg 1992;103:724–32. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical