

Review
doi: 10.1136/heart.89.9.1110.
Development of the heart: (3) formation of the ventricular outflow tracts, arterial valves, and intrapericardial arterial trunks
Affiliations
- PMID: 12923046
- PMCID: PMC1767864
- DOI: 10.1136/heart.89.9.1110
Item in Clipboard
Review
Development of the heart: (3) formation of the ventricular outflow tracts, arterial valves, and intrapericardial arterial trunks
Heart.
2003 Sep.
No abstract available
Figures
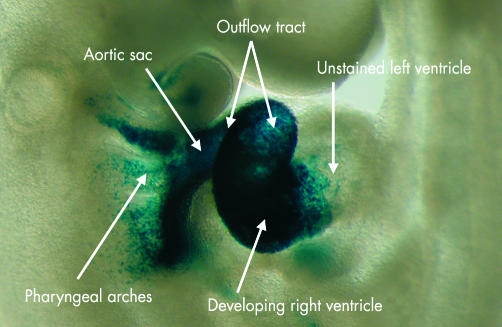
This embryo, viewed from the right side, has been prepared so as to show the product of the transgene for fibroblast growth factor 10 combined with the visualising agent, lacZ. The combined product, now stained blue, marks the contributions made to the developing heart from the secondary heart field. As can be seen, the gene product is found in the pharyngeal arches, the aortic sac, both components of the outflow tract, and the primordium of the developing right ventricle. It does not extend, however, beyond the interventricular groove, the left ventricle being derived from the primary cardiac crescent.
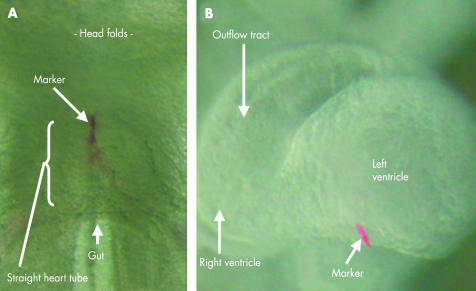
The left hand panel (A) shows an injection of the marker diI placed at the cranial pole of the straight heart tube in a mouse embryo. The embryo was permitted to grow until the tube had looped. Subsequent to looping, as shown in the right hand panel (B), the marker is found proximal to the interventricular groove, showing that the more distal part of the right ventricle and outflow tract have been recruited from a secondary heart field.
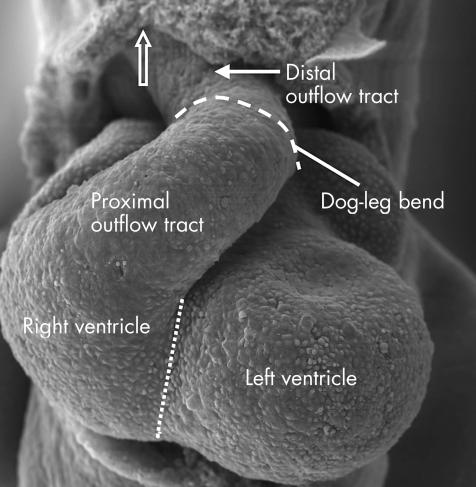
This scanning electron micrograph shows the heart from a mouse with 42 somites. The front of the pericardial cavity has been removed. The outflow tract is supported exclusively by the right ventricle, the dotted line showing the location of the interventricular groove. Note the characteristic bend (dashed line) dividing the outflow tract into proximal and distal portions. Note also that the distal portion extends to the margins of the pericardial cavity (arrow).
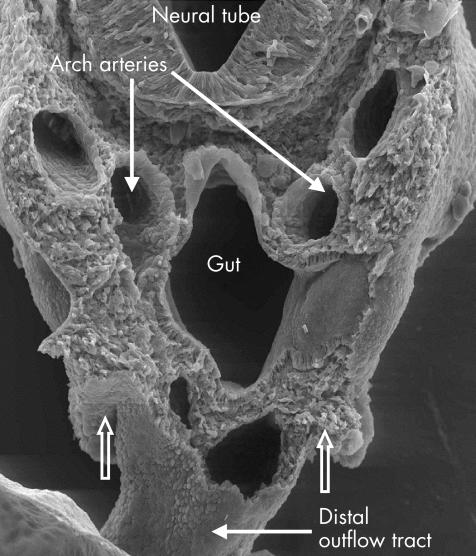
This scanning electron micrograph, again from a mouse with 42 somites, is made by making a transection through the cervical region. It shows the bilateral nature of the arteries extending through the pharyngeal arches at this stage of development. The open arrows show the extent of the pericardial cavity.
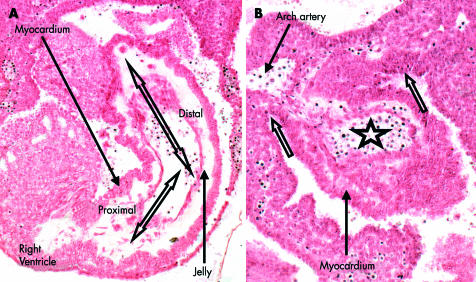
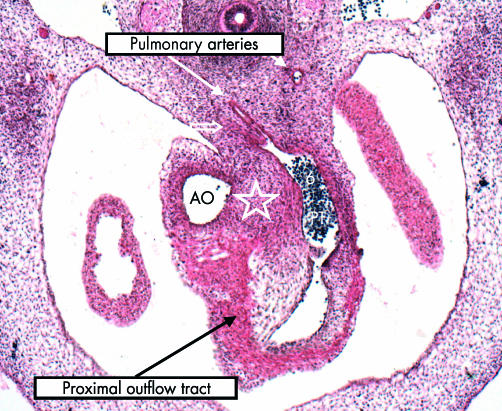
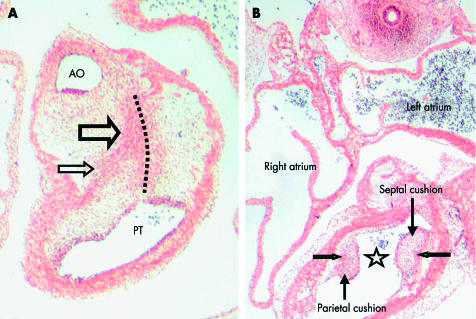
These sections, in the frontal plane, are from a human embryo at the 12th stage of development in the Carnegie categorisation. Panel A shows the proximal and distal parts of the outflow tract, marked by the arrows, with the sharp angulation between them at the dog-leg bend. Both parts, at this stage, have exclusively myocardial walls, the lumen being lined throughout by a layer of endocardial jelly. Panel B shows how the myocardial walls extend to the margins of the pericardial cavity (open arrows), where the lumen of the distal outflow tract (star) becomes continuous with the aortic sac, from which arise the arteries running in the pharyngeal arches (compare with fig 4).
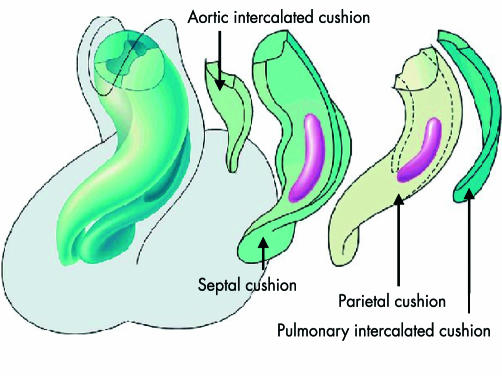
This reconstruction is made from a human embryo at Carnegie stage 15. The main panel, to the left, shows the spiralling nature of the opposing endocardial cushions, or ridges, that extend throughout the length of the outflow tract. The panels to the right show the individual cushions. The major cushions, positioned parietally and septally at their proximal ends, spiral round one another as they extend into the distal outflow tract. The purple zones mark the site of the condensed rods of mesenchyme that have populated the cushions, migrating in from the neural crest. Note also the location of the intercalated cushions, one located anteriorly within the future aortic primordium, and the other posteriorly within the prospective pulmonary outflow tract.
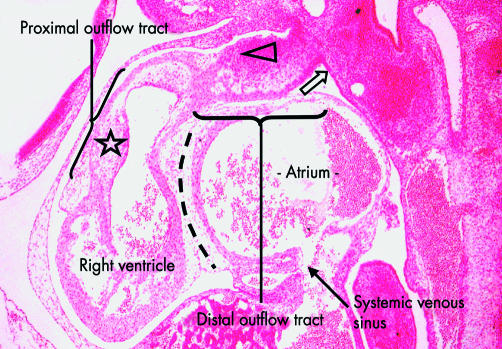
This section, in the sagittal plane, comes from a human embryo at Carnegie stage 15. It shows how the proximal outflow tract is supported exclusively by the developing right ventricle, which at this stage has no direct connection with the developing right atrium (dotted line). Note the proximal parietal cushion (star) in the outflow tract. The distal outflow tract extends to the margin of the pericardial cavity (arrow) and its parietal wall is becoming infiltrated by a densely stained population of cells from the pharyngeal mesenchyme (triangle), with the phenotype of the wall closest to the aortic sac beginning to adopt an arterial rather than myocardial pattern.
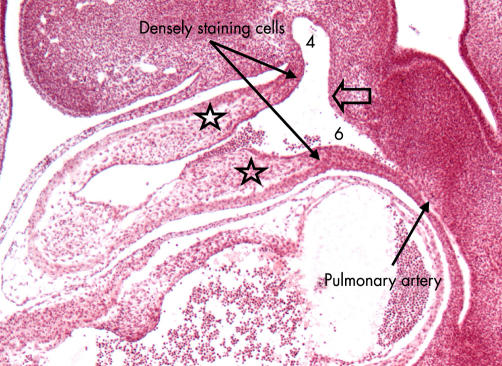
This section, from the same human embryo as shown in fig 7, shows the arrangement of the distal outflow tract. The endocardial jelly has now become organised into cushions, positioned superiorly and inferiorly (stars), which approach each other across the lumen. A further population of densely stained cells, this time derived from the neural crest, is beginning to infiltrate the cushions. Note the arteries to the fourth (4) and sixth (6) pharyngeal arches arising from the aortic sac, and the left pulmonary artery running within the mediastinal mesenchyme. The wedge of mesenchyme between the fourth and sixth arch arteries (arrow) is the so-called aorto-pulmonary septum.
This transverse section through the outflow tract of a human embryo at Carnegie stage 16 shows the differences in maturation between the distal and proximal parts. The distal part has now been separated into the aorta (AO) and pulmonary trunk (PT), the latter continuing into the left sixth aortic arch (6). Note that the right sixth arch (arrow) has now almost involuted. Note also the origin of the right pulmonary artery from the left arch. The cushions that initially septated the distal outflow tract are now no longer recognisable (star), and the walls of the intrapericardial arterial trunks are now developing their arterial phenotype. The proximal outflow tract, in contrast, still possesses a muscular wall, and has cushions in its lumen.
These sections are from the same human embryo, at Carnegie stage 16, as shown in fig 9. The left hand panel (A) sections the outflow tract at the dog-leg bend, which is becoming converted into the sinutubular junctions. Note on the aortic side (AO) that the wall has an arterial phenotype. The cushions have fused at the level of the junction (dotted line), and the central whorl of densely stained mesenchyme is obvious (large arrow), with one of its prongs extending into the parietal cushion (small arrow). The wall of the pulmonary trunk (PT) retains its myocardial phenotype. The right hand panel (B) shows the proximal outflow tract, in which the cushions have still to fuse (star). Note the ends of the prongs of condensed mesenchyme, coloured purple in the reconstruction shown in fig 6, within both cushions (green arrows).
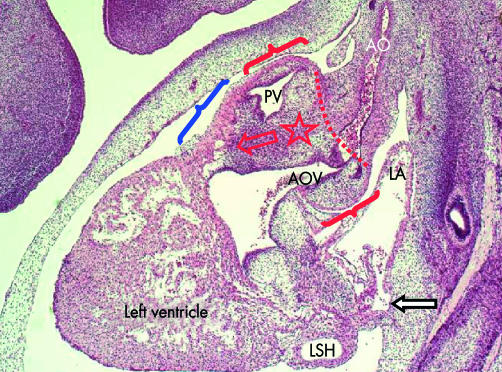
This sagittal section is from a human embryo at Carnegie stage 18. It shows the changes now occurring in the proximal portion of the outflow tract. The dog-leg bend now marks the site of the sinutubular junctions (red dotted line). The intrapericardial part of the aorta (AO) now has its own discrete walls. The distal part of the proximal outflow tract, just below the sinutubular junctions (between red brackets) has now been divided into the developing aortic (AOV) and pulmonary (PV) valves. The condensed mesenchyme now fills the mass of fused cushions (star), with one prong (red arrow) running within the cushion tissues. The proximal outflow tract (blue bracket) still retains its myocardial phenotype. Note the origin of the pulmonary vein (white arrow) inferiorly from the left atrium (LA), and the left sinus horn (LSH) with its own walls in the left atrioventricular groove.
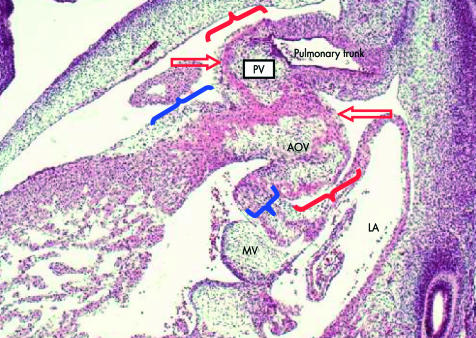
This is another section from the human embryo, at Carnegie stage 18, shown in fig 11. This section shows well the distal (red brackets) and proximal (blue brackets) components of the proximal outflow tract. Note that the proximal part is wedge shaped, with the antero-superior wall longer than the postero-inferior component, albeit that this postero-inferior part is still muscular, and separates the developing leaflets of the aortic (AOV) and mitral (MV) valves. The aortic valve, along with the pulmonary valve (PV) (see fig 13), are beginning to form within the distal part of this proximal component of the outflow tract. The distal outflow tract itself, by now, has transformed into the arterial walls of the aorta and pulmonary trunk, the arterial wall of the pulmonary trunk clearly shown in this section. Both valvar primordiums, derived from the distal end of the proximal outflow tract, are still encased in their muscular walls (red arrows).
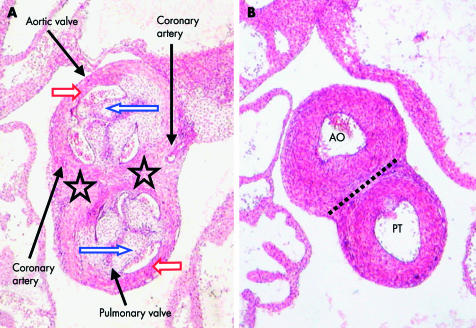
These sections are from a human embryo at Carnegie stage 22, after the interventricular communication has closed. They are cut transversely across the developing arterial valves (A), and the intrapericardial arterial trunks (B). Cavities have now developed in the cushions occupying the distal part of the proximal outflow tract, forming two layers that give rise to the valvar leaflets luminally (blue arrows) and the walls of the supporting sinuses on the mural aspect (red arrows). The mural components are beginning to arterialise. The sinuses and their accompanying leaflets derived from the intercalated cushions, shown by the arrows, form one sinus each for the aorta and pulmonary trunk. The walls of both these sinuses have arterialised, the myocardial covering having disappeared. The myocardium still forms a cuff, however, around the sinuses and leaflets excavated from the fused proximal cushions (stars). Each of the two cushions will contribute one sinus and leaflet to the aorta, and a facing sinus and leaflet to the pulmonary trunk. Note that the coronary arteries will need to perforate the persisting myocardial cuff to enter the aortic sinuses. The second panel (B), taken at a superior level, shows that the intrapericardial parts of the aorta (AO) and pulmonary trunk (PT) now have their distinctive arterial walls. A plane of fibroadipose tissue (dotted line) has appeared between them at the site initially occupied by the distal cushions (see fig 9).
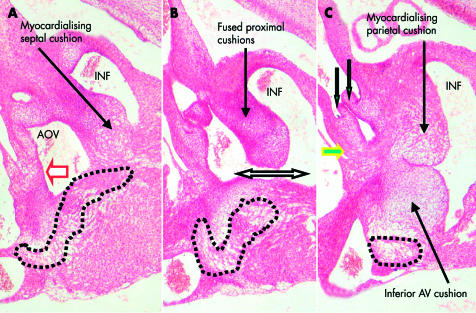
These three panels are from a human embryo at Carnegie stage 20, just at the stage of closure of the embryonic interventricular foramen. The embryo was sectioned in the sagittal plane. The sections illustrate the changes taking place in the proximal part of the proximal outflow tract. Panel A shows the myocardialising septal cushion attached to the muscular ventricular septum immediately above the atrioventricular conduction axis (dotted lines). Note that the posterior aspect of the subaortic vestibule, formed by the initial inner heart curvature, retains its muscular phenotype (red and white arrow). Panel B shows the mid-part of the fused cushions separating the subpulmonary infundibulum (INF) from the subaortic vestibule (AOV). Note the closing interventricular foramen (double headed arrow). Panel C shows the attachment of the myocardialised parietal cushion to the inferior atrioventricular (AV) cushion. Note that the aortic valvar leaflets (white and green arrows), and their developing sinuses, are still enclosed in a myocardial cuff (yellow and green arrows).
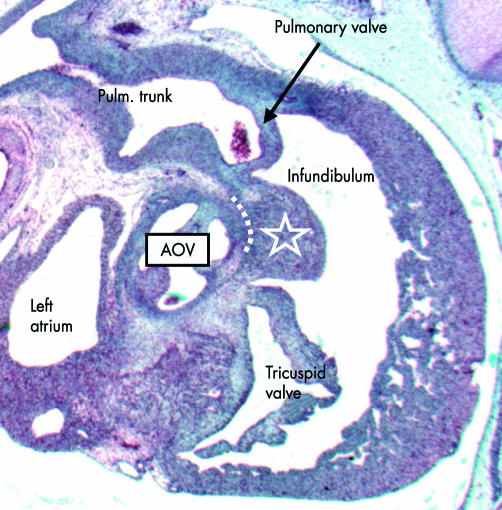
This sagittal section is from a human embryo of 33 mm crown–rump length, at about 8–9 weeks’ gestation. It shows how the myocardialised proximal outflow cushions (white star) are becoming incorporated into the wall of the right ventricle as the supraventricular crest, interposed between the leaflets of the pulmonary and tricuspid valves. With continuing maturation, a tissue plane (dotted line) will develop between the muscularised cushions and the aortic valve (AOV).
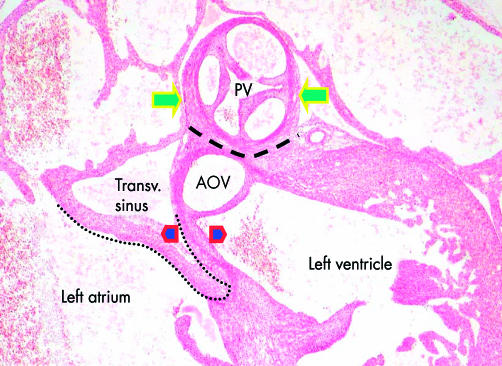
This sagittal section is from a human embryo at Carnegie stage 22, after the completion of cardiac septation. Although a tissue plane (dashed line) has now developed between the pulmonary (PV) and aortic (AOV) valves, the pulmonary valvar sinuses are still enclosed in the cuff of myocardium representing the initial wall of the distal part of the proximal outflow tract (yellow and green arrows). The myocardium still surrounds also the sinuses of the developing aortic valve, here being part of the inner heart curvature (dotted line). After disappearance of the myocardium, the fibrous wall of the aortic root between the hinges of the left and non-coronary aortic leaflets (between red and blue arrow heads) will form a partition between the subaortic outflow tract and the transverse (transv.) sinus of the pericardium. This is one of the three interleaflet triangles of the aortic root.
References
-
- Le Douarin NM. The neural crest. Cambridge: Cambridge University Press, 1982.
-
- Kirby ML, Bockman DE. Neural crest and normal development: a new perspective. Anat Rec 1984;209:1–6. ▸ It was the pioneering work of Le Dourain that first showed the importance of the neural crest in development, but Kirby and her colleagues then extended this work to show the significance of migrations of cells from extracardiac sources to formation of the cardiac outflow tracts and arch arteries. - PubMed
-
- Ya J, van den Hoff MJB, de Boer PAJ, et al. The normal development of the outflow tract in the rat. Circ Res 1998;82:464–72. ▸ The first work to question the conventional division of the outflow tract into “truncus” and “conus”, showing how, during development, there was a retreat of the myocardium initially clothing the entirety of the developing outflow tract. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources