

Comparing the quality of oral anticoagulant management by anticoagulation clinics and by family physicians: a randomized controlled trial
- PMID: 12925422
- PMCID: PMC180652
Comparing the quality of oral anticoagulant management by anticoagulation clinics and by family physicians: a randomized controlled trial
Erratum in
- CMAJ. 2004 Feb 17;170(4):451
Abstract
Background: There is growing evidence that better outcomes are achieved when anticoagulation is managed by anticoagulation clinics rather than by family physicians. We carried out a randomized controlled trial to evaluate these 2 models of anticoagulant care.
Methods: We randomly allocated patients who were expected to require warfarin sodium for 3 months either to anticoagulation clinics located in 3 Canadian tertiary hospitals or to their family physician practices. We evaluated the quality of oral anticoagulant management by comparing the proportion of time that the international normalized ratio (INR) of patients receiving warfarin sodium was within the target therapeutic range +/- 0.2 INR units (expanded therapeutic range) while they were managed in anticoagulation clinics as opposed to family physicians' care over 3 months. We measured the rates of thromboembolic and major hemorrhagic events and patient satisfaction in the 2 groups.
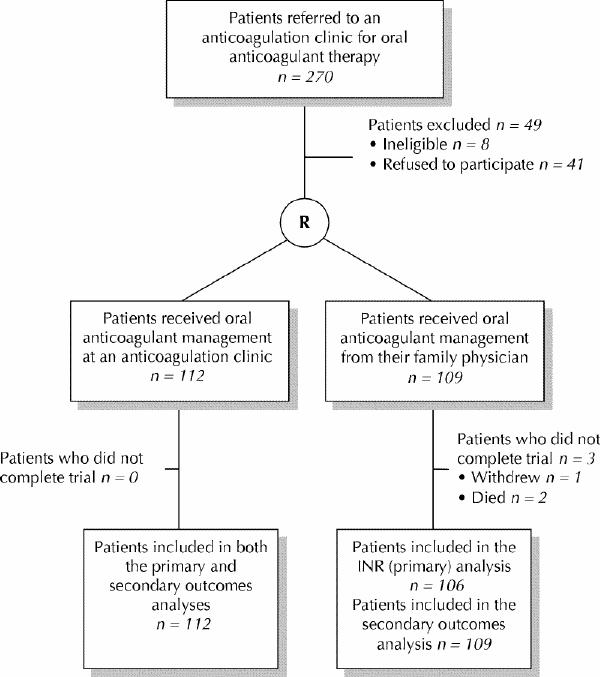
Results: Of the 221 patients enrolled, 112 were randomly assigned to anticoagulation clinics and 109 to family physicians. The INR values of patients who were managed by anticoagulation clinics were within the expanded therapeutic range 82% of the time versus 76% of the time for those managed by family physicians (p = 0.034). High-risk INR values (defined as being < 1.5 or > 5.0) were more commonly observed in patients managed by family physicians (40%) than in patients managed by anticoagulation clinics (30%, p = 0.005). More INR measurements were performed by family physicians than by anticoagulation clinics (13 v. 11, p = 0.001). Major bleeding events (2 [2%] v. 1 [1%]), thromboembolic events (1 [1%] v. 2 [2%]) and deaths (5 [4%] v. 6 [6%]) occurred at a similar frequency in the anticoagulation clinic and family physician groups respectively. Of the 170 (77%) patients who completed the patient satisfaction questionnaire, more were satisfied when their anticoagulant management was managed through anticoagulation clinics than by their family physicians (p = 0.001).
Interpretation: Anticoagulation clinics provided better oral anticoagulant management than family physicians, but the differences were relatively modest.
Figures
Comment in
-
Anticoagulation.CMAJ. 2004 Feb 17;170(4):447, 450; author reply 451. CMAJ. 2004. PMID: 14970077 Free PMC article. No abstract available.
-
Anticoagulation.CMAJ. 2004 Feb 17;170(4):447; author reply 451. CMAJ. 2004. PMID: 14970078 Free PMC article. No abstract available.
-
Anticoagulation.CMAJ. 2004 Feb 17;170(4):447; author reply 451. CMAJ. 2004. PMID: 14970079 Free PMC article. No abstract available.
-
Anticoagulation.CMAJ. 2004 Feb 17;170(4):450; author reply 451. CMAJ. 2004. PMID: 14970081 Free PMC article. No abstract available.
References
-
- Geerts WH, Heit JA, Clagett GP, Pineo GF, Colwell CW, Anderson FA Jr, et al. Prevention of venous thromboembolism. Chest 2001;119(Suppl 1): 132S-75S. - PubMed
-
- Hyers TM, Angelli G, Hull RD, Morris TA, Samama M, Tapson V, et al. Antithrombotic therapy for venous thromboembolic disease. Chest 2001; 119 (Suppl 1):176S-93S. - PubMed
-
- Albers GW, Dalen JE, Laupacis A, Manning WJ, Petersen P, Singer DE, et al. Antithrombotic therapy in atrial fibrillation. Chest 2001;19(Suppl 1):194S-206S. - PubMed
-
- Stein PD, Alpert JS, Bussy HI, Dalen JE, Turpie AGG. Antithrombotic therapy in patients with mechanical and biological prosthetic heart valves. Chest 2001;119(Suppl 1):220S-27S. - PubMed
-
- Cairns JA, Theroux P, Lewis HD, Ezekowitz M, Meade TW. Antithrombotic agents in coronary artery disease. Chest 2001;119(Suppl 1):228S-52S. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical