

Characterization of gene expression profiles associated with glioma progression using oligonucleotide-based microarray analysis and real-time reverse transcription-polymerase chain reaction
- PMID: 12937144
- PMCID: PMC1868272
- DOI: 10.1016/S0002-9440(10)63463-3
Characterization of gene expression profiles associated with glioma progression using oligonucleotide-based microarray analysis and real-time reverse transcription-polymerase chain reaction
Abstract
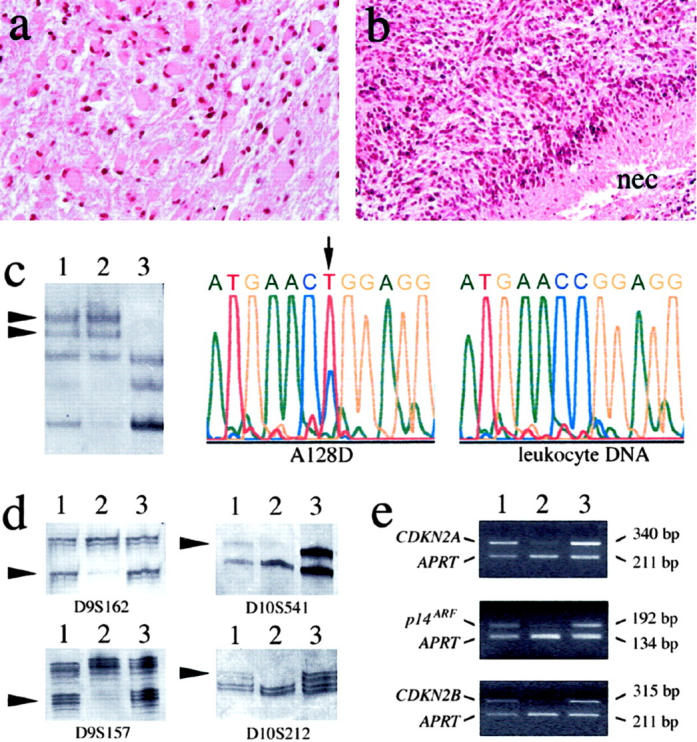
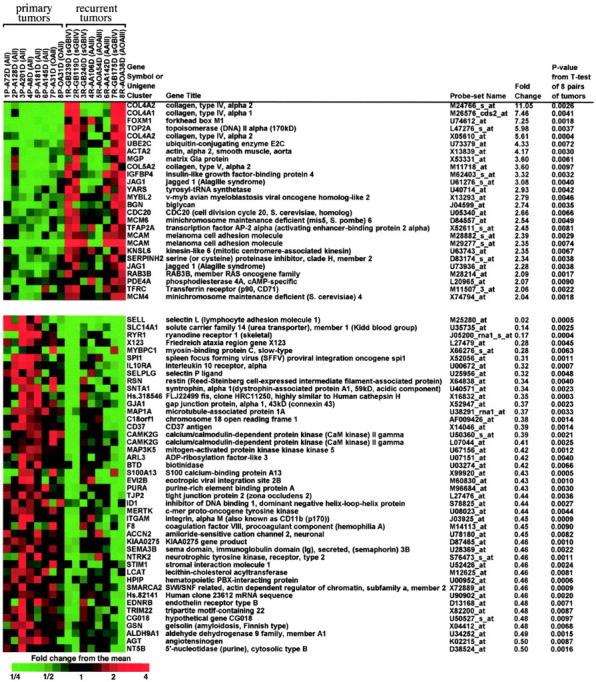
Diffuse astrocytoma of World Health Organization (WHO) grade II has an inherent tendency to spontaneously progress to anaplastic astrocytoma (WHO grade III) and/or glioblastoma (WHO grade IV). The molecular basis of astrocytoma progression is still poorly understood, in particular with respect to the progression-associated changes at the mRNA level. Therefore, we compared the transcriptional profile of approximately 6800 genes in primary WHO grade II gliomas and corresponding recurrent high-grade (WHO grade III or IV) gliomas from eight patients using oligonucleotide-based microarray analysis. We identified 66 genes whose mRNA levels differed significantly (P < 0.01, > or =2-fold change) between the primary and recurrent tumors. The microarray data were corroborated by real-time reverse transcription-polymerase chain reaction analysis of 12 selected genes, including 7 genes with increased expression and 5 genes with reduced expression on progression. In addition, the expression of these 12 genes was determined in an independent series of 43 astrocytic gliomas (9 diffuse astrocytomas, 10 anaplastic astrocytomas, 17 primary, and 7 secondary glioblastomas). These analyses confirmed that the transcript levels of nine of the selected genes (COL4A2, FOXM1, MGP, TOP2A, CENPF, IGFBP4, VEGFA, ADD3, and CAMK2G) differed significantly in WHO grade II astrocytomas as compared to anaplastic astrocytomas and/or glioblastomas. Thus, we identified and validated a set of interesting candidate genes whose differential expression likely plays a role in astrocytoma progression.
Figures

References
-
- Cavenee WK, Furnari FB, Nagane M, Huang HJS, Newcomb EW, Bigner DD, Weller M, Berens ME, Plate KH, Israel MA, Noble MD, Kleihues P: Diffusely infiltrating astrocytomas. Kleihues P Cavenee WK eds. Tumours of the Nervous System. Pathology and Genetics 2000:10-21 IARC Press Lyon
-
- Vertosick FT, Selker RG, Arena VC: Survival of patients with well-differentiated astrocytomas diagnosed in the era of computed tomography. Neurosurgery 1991, 28:496-501 - PubMed
-
- McCormack BM, Miller DC, Budzilovich GN, Voorhees GJ, Ransohoff J: Treatment and survival of low-grade astrocytoma in adults: 1977–1988. Neurosurgery 1992, 31:636-642 - PubMed
-
- Maher EA, Furnari FB, Bachoo RM, Rowitch DH, Louis DN, Cavenee WK, DePinho RA: Malignant glioma: genetics and biology of a grave matter. Genes Dev 2001, 15:1311-1333 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
