

Cervical Spine Stenosis Measures in Normal Subjects
- PMID: 12937434
- PMCID: PMC164344
Cervical Spine Stenosis Measures in Normal Subjects
Abstract
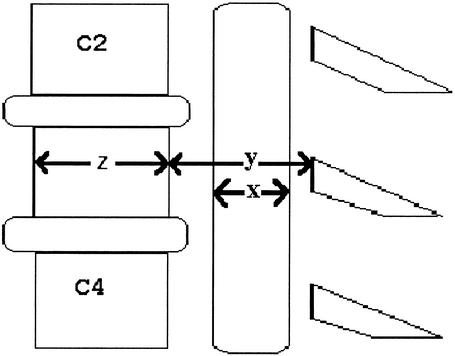
OBJECTIVE: To compare 2 methods of determining cervical spinal stenosis (Torg ratio, space available for the cord [SAC]); determine which of the components of the Torg ratio and the SAC account for more of the variability in the measures; and present standardized SAC values for normal subjects using magnetic resonance imaging (MRI). DESIGN AND SETTING: The research design consisted of a posttest-only, comparison-group design. The independent variable was method of measurement (Torg ratio and SAC). The dependent variables were Torg ratio and SAC scores. SUBJECTS: Fourteen men (age = 24.4 +/- 2.5 years, height = 181.0 +/- 5.8 cm, weight = 90 +/- 13.5 kg) participated in this study. The C3 to C7 vertebrae were examined in each subject (n = 70). MEASUREMENTS: The Torg ratio was determined by dividing the sagittal spinal-canal diameter by the corresponding sagittal vertebral-body diameter. The SAC was determined by subtracting the sagittal spinal-cord diameter from the corresponding sagittal spinal-canal diameter. The Torg ratio and SAC were measured in millimeters. RESULTS: The SAC ranged from 2.5 to 10.4 mm and was greatest at C7 in 71% (10 of 14) of the subjects. The SAC was least at C3 or C5 in 71% (10 of 14) of the subjects. A Pearson product moment correlation revealed a significant relationship between the Torg ratio and SAC (r =.53, P <.01). Regression analyses revealed the vertebral body (r (2) =.58) accounted for more variability in the Torg ratio than the spinal canal (r (2) =.48). Also, the spinal canal (r (2) =.66) accounted for more variability in the SAC than the spinal cord (r (2) =.23). CONCLUSIONS: The SAC measure relies more on the spinal canal compared with the Torg ratio and, therefore, may be a more effective indicator of spinal stenosis. This is relevant clinically because neurologic injury related to stenosis is a function of the spinal canal and the spinal cord (not the vertebral body). Further research must be done, however, to validate the SAC measure.
Figures
References
-
- Torg J S, Corcoran T A, Thibault L E, et al. Cervical cord neurapraxia: classification, pathomechanics, morbidity, and management guidelines. J Neurosurg. 1997;87:843–850. - PubMed
-
- Grant T T, Puffer J. Cervical stenosis: a developmental anomaly with quadriparesis during football. Am J Sports Med. 1976;4:219–221. - PubMed
-
- Hashimoto I, Tak Y K. The true sagittal diameter of the cervical spinal canal and its diagnostic significance in cervical myelopathy. J Neurosurg. 1977;47:912–916. - PubMed
-
- Torg J S, Pavlov H, Genuario S E, et al. Neurapraxia of the cervical spinal cord with transient quadriplegia. J Bone Joint Surg Am. 1986;68:1354–1370. - PubMed
-
- Torg J S, Naranja R J, Jr, Pavlov H, Talinat B J, Warren R, Stine R A. The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am. 1996;78:1308–1314. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous